What is Hiatus Hernia?
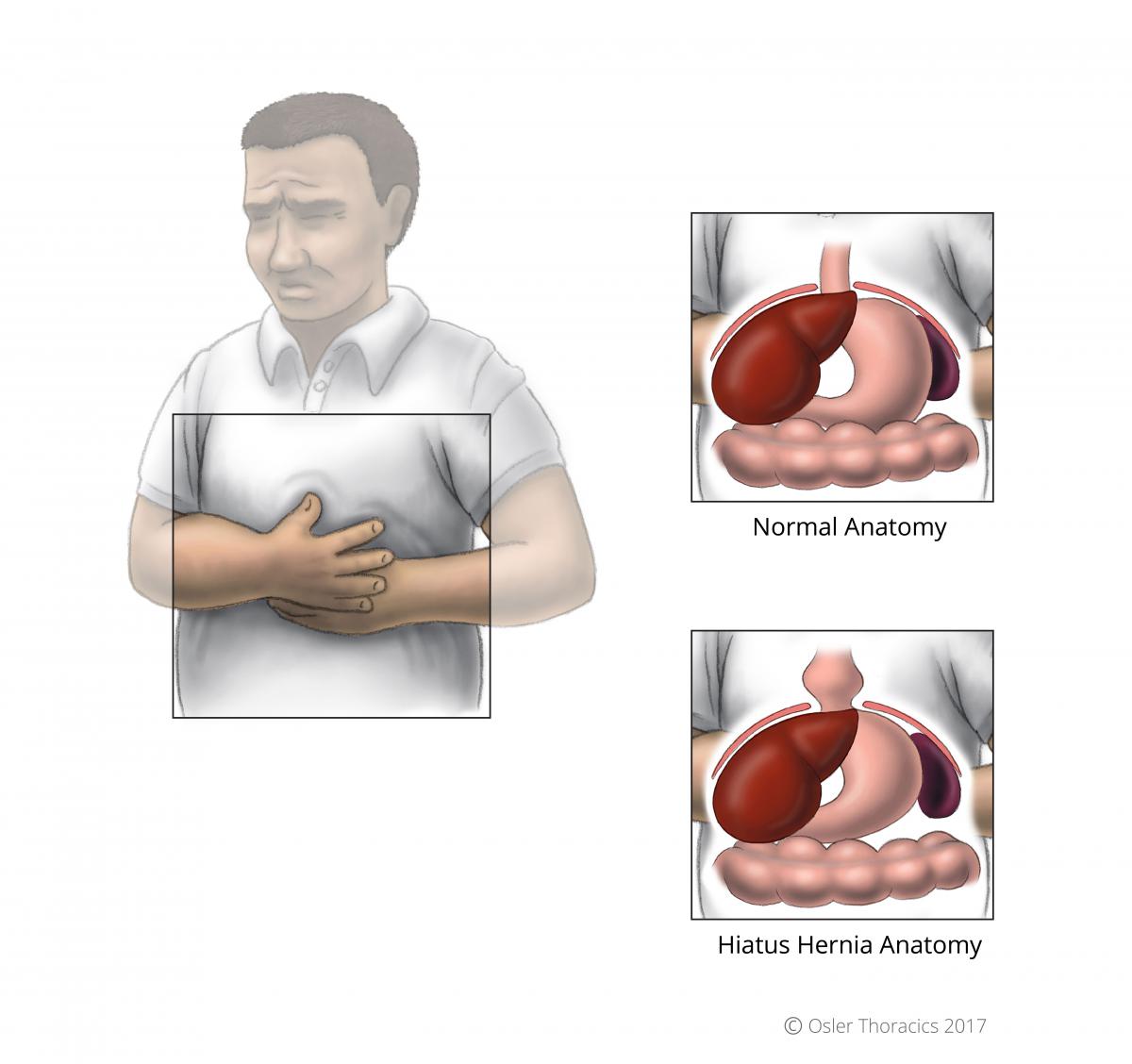
Between your chest and your abdomen, there is a large, flat muscle called the diaphragm. One of its functions is to separate your chest from your abdomen, and keep everything where it belongs! There is a small hole in your diaphragm called the esophageal hiatus that allows the esophagus to connect with your stomach. Hiatal hernias occur when the opening of the diaphragm becomes enlarged, allowing the stomach or other abdominal organs to protrude into the chest. Although hiatus hernias may sound daunting, many of them do not need to be repaired.
What Are the Symptoms?
There are many symptoms of hiatus hernia. They include:
- Abdominal pain
- Bloating
- Trouble getting food down
- Vomiting
- Heartburn
Symptoms are often worse when leaning forward or laying flat.
When Do We Operate?
At William Osler Health System we operate on patients with hiatus hernias who have:
- Symptomatic hiatus hernias
- Very large hiatus hernias
- Hiatus hernias that have a partial twist of the stomach, called a gastric volvulus (which can be life-threatening)
- Chronic anemia with small ulcerations in the stomach. The diaphragm can put pressure on the stomach wall leading to Cameron Ulcers, which can be painful and bleed.
- Symptoms that are well controlled with medication, however the patient does not want to depend on oral medications for the rest of their life
- Symptoms that are not adequately controlled by medication
Other symptoms of hiatus hernias include belching, and regurgitation of bitter tasting fluid. Atypical symptoms include coughing, asthma, or other breathing difficulties. In fact, the most common cause of adult onset asthma in unrecognized hiatus hernias with gastroesophageal reflux. Very large hernias may cause difficulty breathing if the stomach presses into the chest and prevents the lungs from filling normally. Hiatal hernia repair involves pulling the abdominal organs out of the chest and back into the abdominal cavity.
Hiatus Hernia Repair 1
Through 5 small incisions, the enlarged hiatus in the diaphragm is closed with non-dissolvable sutures.
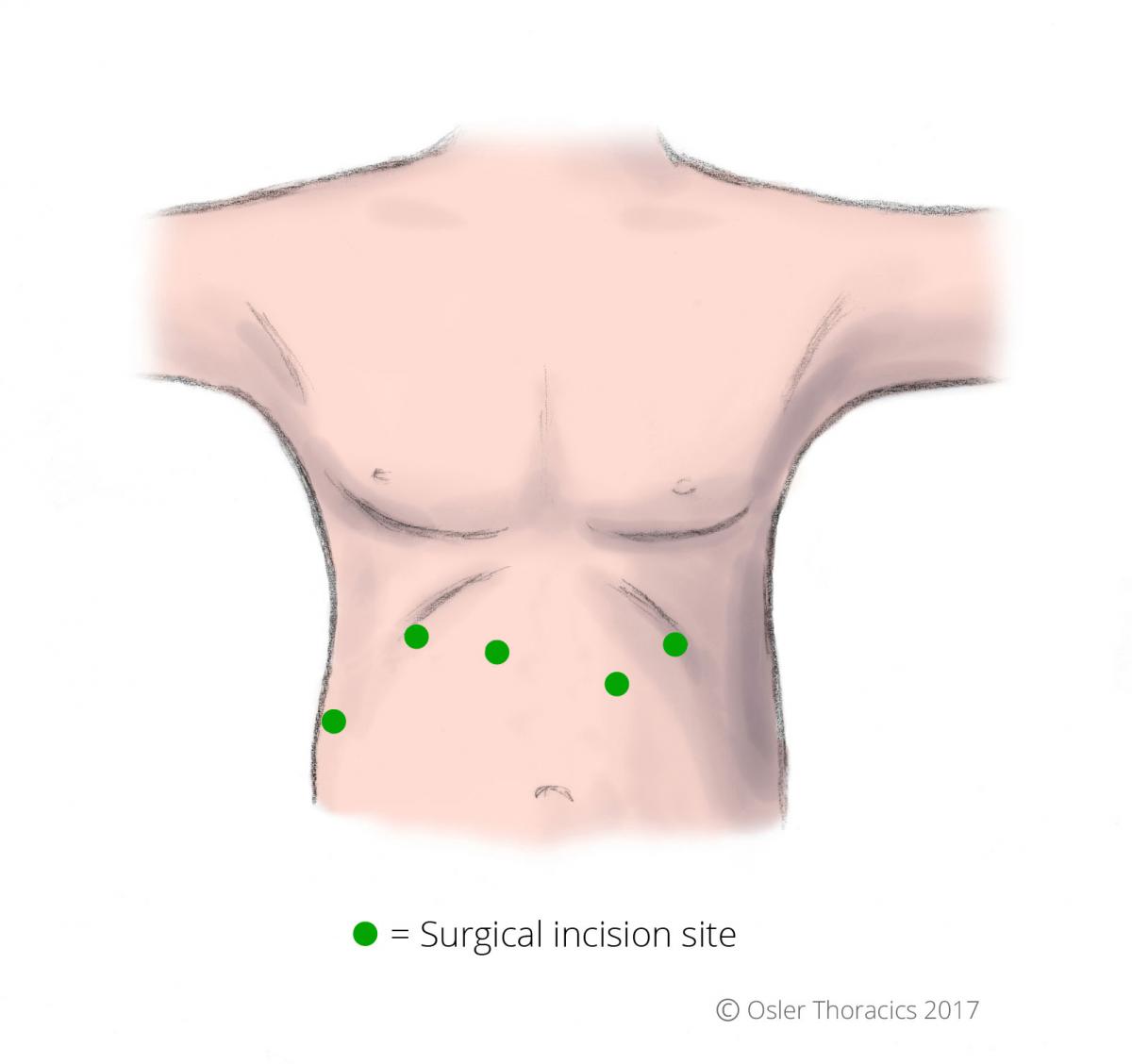
Figure 2: Location of laparoscopic surgical incision sites with hiatus hernia repair surgery
To prevent the stomach from moving back into the chest a portion of the stomach is wrapped around the lower part of the esophagus. This is called a fundoplication, and it prevents the stomach from slipping back into the chest and also prevents acid from refluxing into the esophagus.
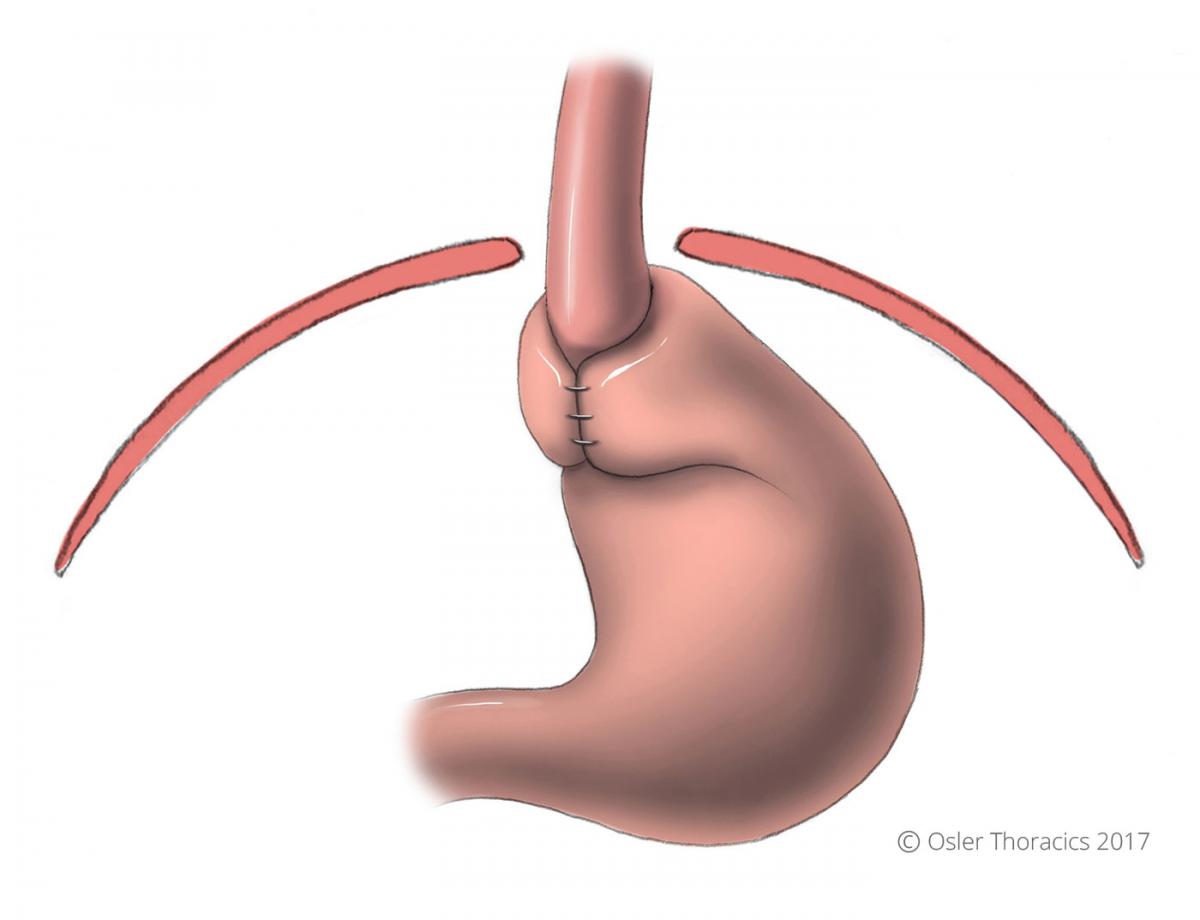
Figure 3: A fundoplication keeps the stomach below the diaphragm, and in the abdomen
Most hiatal hernia surgery is done as an elective procedure and requires you to stay in the hospital overnight. You will usually have an x-ray swallowing study done the morning after surgery and, if the study is normal, be advanced to an oral diet before being sent home. You will have specific diet restrictions after reflux surgery and will be seen by a registered dietician before your discharge.
Before Your Surgery (Pre-Op)
Tests Before Your Surgery
Osler’s Thoracic Surgeons will assess you in the clinic situated next to the Brampton Civic Hospital. You will likely have an endoscopy done, which looks directly into your esophagus and stomach. Your surgeon may also order a barium swallow which provides a nice image of your esophageal and gastric (stomach) anatomy.

Figure 4: An image from a barium swallow; notice the large hiatus hernia above the diaphragm and in the chest On occasion a 24-hour pH and manometry study will be requested. Unfortunately, there are not many centers in the GTA that offer this test, so there may be a long wait-time. This study involves a small pH sensor placed into your esophagus that takes measurements of the acid levels in your stomach throughout one day.
The probe is small, and the end of it is lightly taped to your nose. The probe measures:
- The number of episodes of reflux you have
- The total time the acid level is too high in your esophagus
- How high in the esophagus the acid reaches
- Whether your symptoms correlate with acid spikes
This study provides us with a number called the DeMeester Score. A score over 15 is usually diagnostic for significant reflux.
This study is not always possible or reliable in large hiatal hernias because it is difficult to place the sensors in the proper locations.
The pressures of your esophagus will also be measured (manometry). If the esophagus does not contract properly, your surgeon may not perform the anti-reflux portion of your hiatal hernia repair or perform a variation of the fundoplication that leaves the wrap around the esophagus looser than normal.
Meeting With Your Surgeon
After these tests are completed, the thoracic surgeon will have a discussion with you about whether surgical repair is recommended.
If both you and the thoracic surgeon agree to proceed with surgery, the operation date will be booked.
You will also have a detailed discussion with your surgeon about the risks and benefits of reflux surgery, including the small possibility that your symptoms will not get better, or that you may need to continue taking medications to help control your symptoms.
This is a great opportunity to ask as many questions as you want.
After Your Surgery (Post-Op)
How Long Will I Stay in Hospital?
After these tests are completed, the thoracic surgeon will have a discussion with you about whether surgical repair is recommended.
If both you and the thoracic surgeon agree to proceed with surgery, the operation date will be booked.
You will also have a detailed discussion with your surgeon about the risks and benefits of reflux surgery, including the small possibility that your symptoms will not get better, or that you may need to continue taking medications to help control your symptoms.
This is a great opportunity to ask as many questions as you want.
How Long Will I Stay in Hospital?
After your surgery, you will stay in the hospital overnight and likely be discharged the next day.
You will have a swallowing study done the morning after surgery. If the swallow study is normal, you will be given a liquid diet and you will start preparing to go home. The dietician will also sit and talk with you about our post-hiatus hernia diet. The doctor will then be able to discharge you home later in the early afternoon.
How Will I Feel Post-Op?
Normal Symptoms After a Hiatus Hernia Repair:
- Pain (you may feel pain where your incisions are, especially during movement)
- Abdominal bloating
- Trouble swallowing large bites of food (food will get stuck but can be washed down with water)
- Inability to burp or vomit easily
The fundoplication prevents acid from moving up into your esophagus. However, for a few weeks after surgery surgical, swelling may make the wrap too snug. This may cause some food hold-up, and may also prevent you from burping which can lead to bloating. These symptoms typically resolve in 6-8 weeks. If they have not, please contact your surgeon’s office.
Contact Your Surgeon If:
- You have a fever of 101°F or higher: This could be a sign of infection
- You have redness around your incisions: This could be a sign of skin infection or deeper infection
- You have drainage from your incisions, particularly if it is thick and foul smelling: This could be a sign of a deeper infection
- You have nausea*, vomiting, or abdominal distention (bloating) that is not controllable
- You develop worsening swelling in your legs or have sudden shortness of breath (this could be a sign of blood clots)
- You have severe pain with swallowing or in your stomach after eating
- Food “sticks” in the lower part of your esophagus, and you can’t wash it down with water
- Your pain gets worse or is not relieved by your prescription pain medications
- You are not making urine as you were before your operation
- You have shortness of breath and/or chest pain
*It is very important to control any nausea you might experience after your surgery. Retching or vomiting strains the surgical site, which can cause complications. Please let your surgeon know if you develop nausea after discharge so that he or she can address this further.
What Kind of Activity Can I Do?
At the Hospital
The evening of your surgery, we will have you sitting in a chair and walking in the hallway. Being active reduces the risk of blood clots, and improves your breathing to prevent pneumonia. The nursing staff on the surgical ward will insist on getting you out of bed!
At Home
Household Activities: After discharge from the hospital, avoid lifting more than 15 pounds for at least 4 weeks, and avoid excessive bending or twisting for 2 weeks following surgery. We also suggest you avoid household activities like vacuuming, carrying groceries, or shoveling snow for at least 4 weeks. Every time you lift or push heavy objects, you strain the hiatus. Although this usually isn’t a problem, repeated force may undo all the work that was done.
Driving
Avoid driving until you no longer need narcotic pain medication and you feel you can make rapid movements unimpaired by pain. Driving while taking narcotics can impair your ability to drive safely.
Work
You should be able to return to work in 2-3 weeks. If your job involves heavy lifting and light duty is not an option, you may need up to 4 weeks off work to recover.
Sports
We suggest avoiding sports for 4 weeks. You can go for brisk walks 10 days after surgery. Wait 2 weeks before you swim.
Taking Care of Your Incisions
When Can I Remove the Dressings?
All the hiatus hernias we operate on are repaired laparoscopically. A small white dressing is typically placed over each incision. These dressings may be removed 48 hours (2 days) after the operation.
Below this dressing are small brown or white pieces of tape (called Steri-Strips™); these will fall off on their own within 1-2 weeks. If they don’t fall off, you can remove them in the shower after two weeks.
If your surgeon gives you specific instructions other than this, please follow those instructions.
Bathing
You can shower 48 hours after the surgery (after the gauze and clear tape dressing is removed). It is okay to get soap and water on the incisions. Pat the area dry.
We recommend that you don’t submerge yourself in water (in a bathtub, pool, or hot-tub) for at least two weeks post-op.
When to Contact Your Doctor
If you notice drainage from your incisions, particularly if it is thick and foul-smelling or associated with a fever, contact your surgeon immediately.
If you notice redness around your incisions, especially if it is getting worse or associated with drainage or a fever, contact your surgeon.
Pain Management and Medication
Although your surgery was likely completed using keyhole incisions you may have some pain. You will be given a PCA, a patient controlled analgesia, which allows you to press a button for additional medication when you need it.
At Osler we have an “Acute Pain Service” that is supervised by an anesthesiologist and a nurse practitioner. They will see you a few times to make sure you are comfortable. Sometimes after hiatus hernia surgery patients complain of left shoulder pain. This is from the sutures that we use to reconstruct the muscle defect of the diaphragm and some retained air in your abdominal cavity. Pain from air inflation will go away in 24 to 48 hours.
Your pain should be controlled well enough for you to begin getting out of bed the morning after surgery.
You will be discharged with pain medication, typically a mild to moderate strength narcotic. Take as needed and as prescribed.
Other Medications
You will be prescribed a stool softener when you go home. Narcotic or pain medications can cause constipation and a stool softener may help. If you have some nausea at home, you can pick up some Gravol® from the pharmacy.
Your Regular Medications
Unless otherwise instructed, continue to take your usual home medications once you are home.
Osler’s Post Hiatus Hernia Dietary Guidelines
Following hiatus hernia repair, you will need to follow a special diet for at least 6 weeks. The foods included in this diet will pass more easily through your digestive system, promote faster healing from surgery, and prevent possible complications.
You may leave the hospital on a full fluid diet and it is recommended that you stay on this diet for 2-3 days from your surgery date. Below are examples of the diet you may follow post-op. Most patients can progress to a
The exact timeframe of diet progression will depend on your individual tolerance, and your surgeon's recommendations
General Dietary Guidelines
- Eat and drink slowly
- Chew food well: follow the rule of 25- chew each bite of solid food 25 times before swallowing
- Avoid gulping
- Minimize using a straw
- Minimize consuming carbonated beverages (soda, beer, sparkling water, etc.): These can cause severe bloating
- Caffeinated beverages in moderation
- Minimize chewing gum
- Eat foods that are easy to digest (soft, moist foods)
- Avoid gas producing foods (i.e. beans, cabbage, onions) as you transition to a regular diet
- Remain upright while eating
- Avoid laying down for at least 30 minutes after eating
- Eat smaller portions (½ cup -¾ cup per meal initially), and eat more frequent meals and snacks rather than large meals
- Add ½ cup (125ml) nutritional supplement high protein* with each meal during the first 2 weeks after surgery especially when on a fluid diet (at least 6 servings per day)
*Examples of high-protein nutritional supplements are: Ensure® High Protein, Boost® High Protein, Equality High Protein, And Carnation Breakfast Essential.
Sample Diets
Day 1-5: Fluids and Semi Fluids Diet Guidelines
This diet can be followed up to the first week after surgery.
Full fluids are pourable, smooth, with no lumps and include the following:
- Juice (fruit and vegetable)
- Broth or consommé
- Jell-O
- Popsicles and Italian ice
- Milk
- Yogurt (without fruit pieces)
- Pudding
- Ice cream (without candy pieces, nuts, or fruit chunks)
- Milkshakes
- Strained cream soups
- Nutritional supplement drinks (Boost®, Ensure®, Carnation Instant Breakfast)
Week 1-2: Pureed/Blenderized Diet Guidelines
Pureed foods have a smooth texture. In addition to all foods on the full liquid diet you may add the following:
- Blenderized meat, dhal, chicken, fish, etc.
- Blenderized vegetables
- Applesauce and other pureed fruits
- Mashed potatoes
- Egg custard
- Cream of wheat and other cooked cereals
Week 3-6: Soft Diet Guidelines
Foods included on a soft diet have a mushy texture and are easy to digest. The foods recommended on a soft diet are:
- Grains: Well cooked pasta, noodles, moist rice, cooked cereal
- Vegetables: Well cooked, soft vegetables
- Fruits: Canned fruit, bananas, melon
- Milk Products: Milk, yogurt, soft cheeses, cottage cheese, ice cream, pudding, custard
- Protein Foods: Moist meats with gravy, moist fish, soft cooked eggs, tofu
- Fats: Butter, margarine, mayonnaise, salad dressing, cream
- Other: Jell-O, Italian ice, popsicles, sherbet, sorbet
- Beverages: Fruit and vegetable juice, non-carbonated soft drinks
Foods NOT recommended on a soft diet:
- Grains: Bread, dry cereal, crackers, chips, popcorn
- Vegetables: Raw vegetables, corn
- Fruits: Dried fruit, fresh fruit with skins
- Milk Products: Ice cream with nuts, candy pieces or fruit chunks
- Protein Foods: Nuts and seeds, peanut butter, dry meats
- Fats: Crispy fried foods
- Other: Candy, cookies, crusts, dry cakes and pastries
- Beverages: Alcohol
Sample Soft Diet Menu
An example of what you might eat in a day following the soft diet is below:
Breakfast
- 2 eggs, scrambled
- ¾ cup oatmeal with milk
- ¾ cup fruit juice
Snack
- 8 oz. vanilla yogurt
- 1 banana, mashed
Lunch
- 1 cup macaroni and cheese
- ½ cup cooked peas
- ¾ cup vegetable juice
Dinner
- 4 oz. moist cooked salmon
- ½ cup mashed potatoes with gravy
- ½ cup cooked green beans
Snack
- ½ cup cottage cheese
- ½ cup canned peaches
You can include any non-carbonated, caffeine-free beverages with your meals
Follow-Up
You will be given a date and time to see your surgeon following surgery, usually in 3 weeks. T
he follow-up appointment should have been arranged during the office visit. If not, please call 905-458-4520 to arrange an appointment.