What is a Esophageal Cancer?
Esophageal cancer is a disease in which malignant (cancer) cells form in the tissues of the esophagus.
The esophagus is the hollow, muscular tube that moves food and liquid from the throat to the stomach. The wall of the esophagus is made up of several layers of tissue, including mucous membrane, muscle, and connective tissue. Esophageal cancer starts on the inside lining of the esophagus and spreads outward through the other layers as it grows.
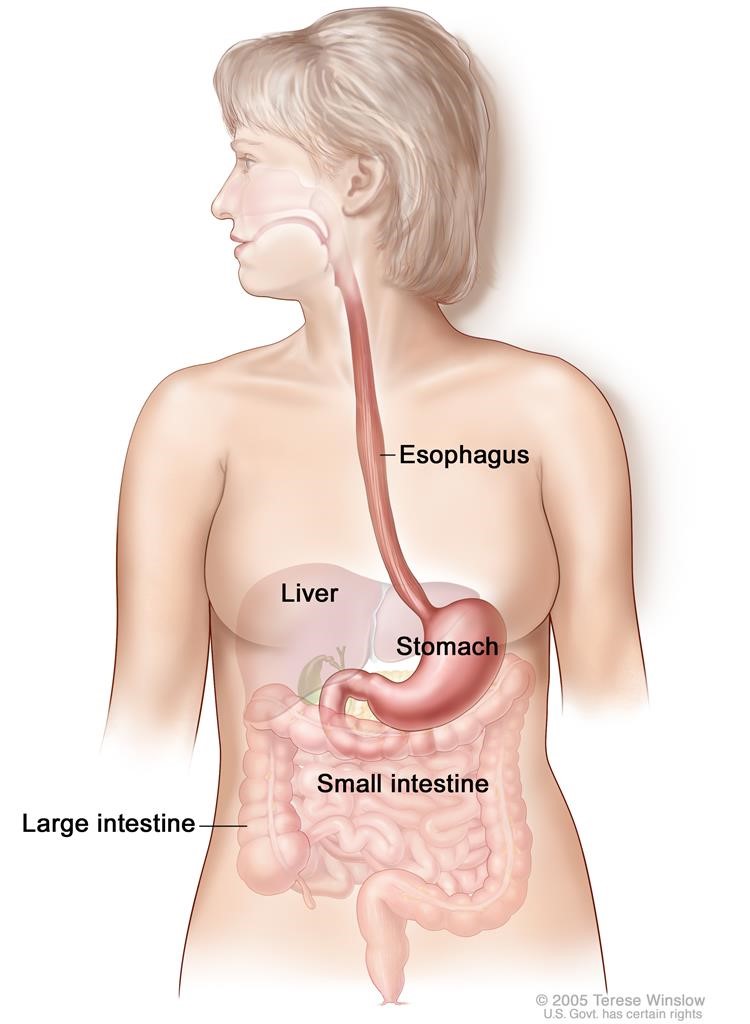
Figure 1: The esophagus and stomach are part of the upper gastrointestinal (digestive) system.
The two most common forms of esophageal cancer are named for the type of cells that become malignant (cancerous):
- Squamous cell carcinoma: Cancer that forms in squamous cells, the thin, flat cells lining the esophagus. This cancer is most often found in the upper and middle part of the esophagus, but can occur anywhere along the esophagus. This is also called epidermoid carcinoma.
- Adenocarcinoma: Cancer that begins in glandular (secretory) cells. Glandular cells in the lining of the esophagus produce and release fluids such as mucus. Adenocarcinomas usually form in the lower part of the esophagus, near the stomach.
Smoking, heavy alcohol use, and Barrett esophagus can increase the risk of esophageal cancer. Anything that increases your risk of getting a disease is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors doesn't mean that you will not get cancer. Talk with your doctor if you think you may be at risk. Risk factors include the following:
- Tobacco use.
- Heavy alcohol use.
- Barrett esophagus: A condition in which the cells lining the lower part of the esophagus have changed or been replaced with abnormal cells that could lead to cancer of the esophagus. Gastric reflux (the backing up of stomach contents into the lower section of the esophagus) may irritate the esophagus and, over time, cause Barrett esophagus.
- Older age.
Tests that examine the esophagus are used to detect (find) and diagnose esophageal cancer.
Certain factors affect prognosis (chance of recovery) and treatment options.
Recurrent Esophageal Cancer:
Recurrent esophageal cancer is cancer that has recurred (come back) after it has been treated. The cancer may come back in the esophagus or in other parts of the body.
What Are the Symptoms?
Some symptoms of esophageal cancer are:
- Weight loss
- Pain swallowing
- Difficulty swallowing
It is recommended that you check with your doctor if you also experience any of the following:
- Pain behind your breastbone
- Hoarseness and a cough
- Indigestion and heartburn
What Tests Can be Used to Detect / Diagnose Esophageal Cancer?
Tests that examine the esophagus are used to detect (find) and diagnose esophageal cancer.
The following tests and procedures may be used:
- Physical exam and history : An exam of the body to check general signs of health, including checking for signs of disease, such as lumps or anything else that seems unusual. A history of the patient’s health habits and past illnesses and treatments will also be taken.
- Chest x-ray : An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body.
- Barium swallow : A series of x-rays of the esophagus and stomach. The patient drinks a liquid that contains barium (a silver-white metallic compound). The liquid coats the esophagus and stomach, and x-rays are taken. This procedure is also called an upper GI series.

Figure 2: Barium swallow. The patient swallows barium liquid and it flows through the esophagus and into the stomach. X-rays are taken to look for abnormal areas.
Esophagoscopy : A procedure to look inside the esophagus to check for abnormal areas. An esophagoscope is inserted through the mouth or nose and down the throat into the esophagus. An esophagoscope is a thin, tube-like instrument with a light and a lens for viewing. It may also have a tool to remove tissue samples, which are checked under a microscope for signs of cancer. When the esophagus and stomach are looked at, it is called an upper endoscopy.
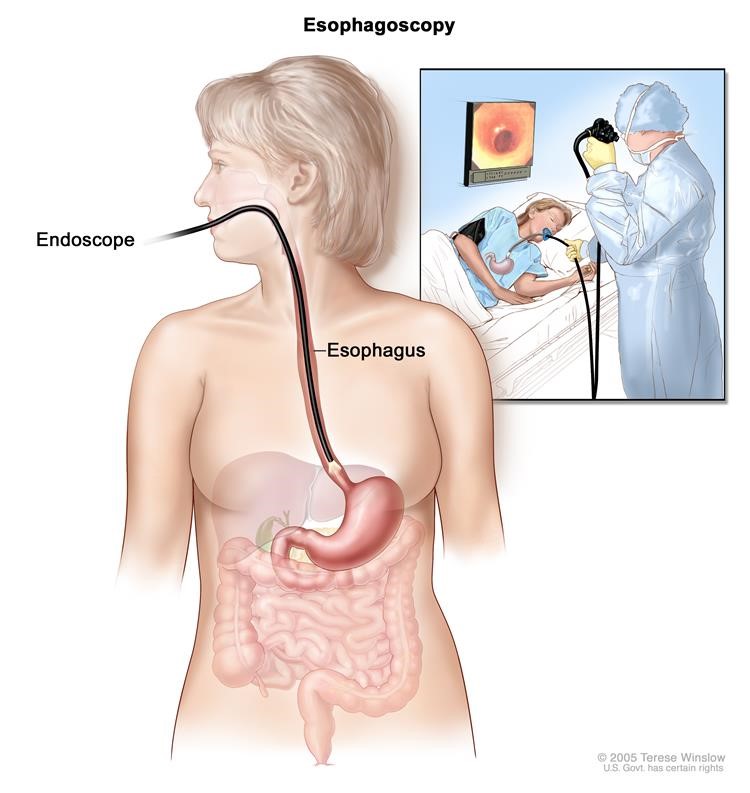
Figure 3: Esophagoscopy. A thin, lighted tube is inserted through the mouth and into the esophagus to look for abnormal areas.
- Biopsy : The removal of cells or tissues so they can be viewed under a microscope by a pathologist to check for signs of cancer. The biopsy is usually done during an esophagoscopy. Sometimes a biopsy shows changes in the esophagus that are not cancer but may lead to cancer.
When Do We Operate?
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis (chance of recovery) and treatment options depend on the following:
- The stage of the cancer (whether it affects part of the esophagus, involves the whole esophagus, or has spread to other places in the body).
- Whether the tumor can be completely removed by surgery.
- The patient’s general health.
When esophageal cancer is found very early, there is a better chance of recovery. Esophageal cancer is often in an advanced stage when it is diagnosed. At later stages, esophageal cancer can be treated but rarely can be cured. Taking part in one of the clinical trials being done to improve treatment should be considered. Information about ongoing clinical trials is available from the NCI website.
Many people with esophageal cancer find it hard to eat because they have trouble swallowing. The esophagus may be narrowed by the tumor or as a side effect of treatment. Some patients may receive nutrients directly into a vein. Others may need a feeding tube (a flexible plastic tube that is passed through the nose or mouth into the stomach) until they are able to eat on their own.
Criteria For Surgical Repair
Minimally-Invasive Esophagectomy
Surgery is the most common treatment for cancer of the esophagus. Part of the esophagus may be removed in an operation called an esophagectomy.
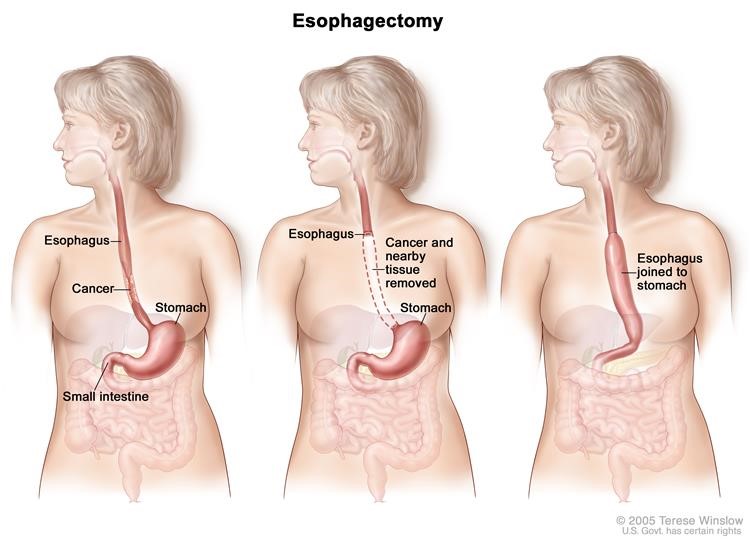
Figure 4: Esophagectomy. A portion of the esophagus is removed and the stomach is pulled up and joined to the remaining esophagus.
The doctor will connect the remaining healthy part of the esophagus to the stomach so the patient can still swallow. A plastic tube or part of the intestine may be used to make the connection. Lymph nodes near the esophagus may also be removed and viewed under a microscope to see if they contain cancer. If the esophagus is partly blocked by the tumor, an expandable metal stent (tube) may be placed inside the esophagus to help keep it open.
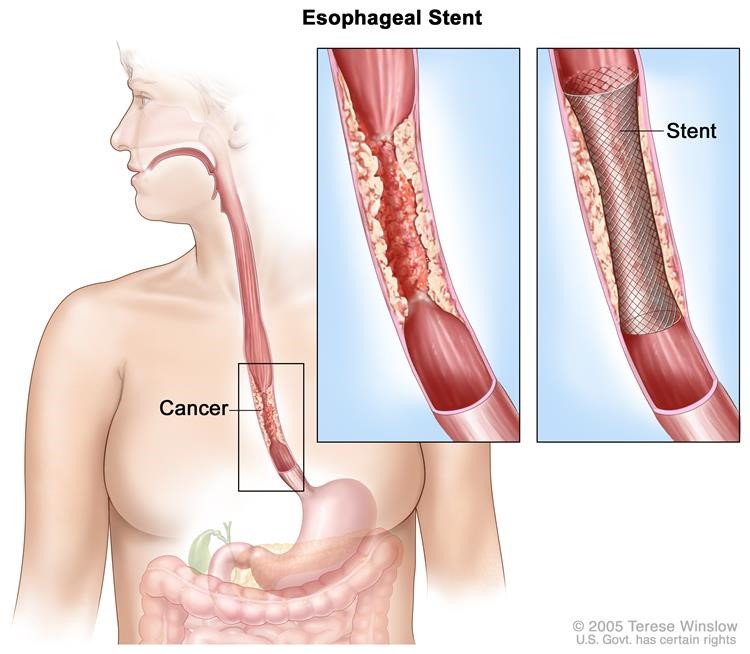
Figure 5: Esophageal stent. A device (stent) is placed in the esophagus to keep it open to allow food and liquids to pass through into the stomach.
Small, early-stage cancer and high-grade dysplasia of the esophagus may be removed by endoscopic resection. An endoscope (a thin, tube-like instrument with a light and a lens for viewing) is inserted through a small incision (cut) in the skin or through an opening in the body, such as the mouth. A tool attached to the endoscope is used to remove tissue.
Advantages of the Esophageal Cancer
Disadvantages of the Esophageal Cancer
Before Your Surgery (Pre-Op)
Tests Before Your Surgery
The process used to find out if cancer cells have spread within the esophagus or to other parts of the body is called staging. The information gathered from the staging process determines the stage of the disease. It is important to know the stage in order to plan treatment. The following tests and procedures may be used in the staging process:
Endoscopic ultrasound (EUS)
A procedure in which an endoscope is inserted into the body, usually through the mouth or rectum. For esophageal cancer, the endoscope is inserted through the mouth. An endoscope is a thin, tube-like instrument with a light and a lens for viewing. A probe at the end of the endoscope is used to bounce high-energy sound waves (ultrasound) off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram. This procedure is also called endosonography.
CT scan (CAT scan)
A procedure that makes a series of detailed pictures of areas inside the body, such as the chest, abdomen, and pelvis, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injectedinto a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
PET scan (positron emission tomography scan)
A procedure to find malignant tumorcells in the body. A small amount of radioactive glucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do. A PET scan and CT scan may be done at the same time. This is called a PET-CT.
MRI (magnetic resonance imaging)
A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. This procedure is also called nuclear magnetic resonance imaging (NMRI).
Thoracoscopy
A surgical procedure to look at the organs inside the chest to check for abnormal areas. An incision (cut) is made between two ribs and a thoracoscope is inserted into the chest. A thoracoscope is a thin, tube-like instrument with a light and a lens for viewing. It may also have a tool to remove tissue or lymph node samples, which are checked under a microscope for signs of cancer. In some cases, this procedure may be used to remove part of the esophagus or lung.
Laparoscopy
A surgical procedure to look at the organs inside the abdomen to check for signs of disease. Small incisions (cuts) are made in the wall of the abdomen and a laparoscope (a thin, lighted tube) is inserted into one of the incisions. Other instruments may be inserted through the same or other incisions to perform procedures such as removing organs or taking tissue samples to be checked under a microscope for signs of disease.
Staging Esophageal Cancer
There are three ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
Cancer may spread from where it began to other parts of the body.
When cancer spreads to another part of the body, it is called metastasis. Cancer cells break away from where they began (the primary tumor) and travel through the lymph system or blood.
- Lymph system. The cancer gets into the lymph system, travels through the lymph vessels, and forms a tumor (metastatic tumor) in another part of the body.
- Blood. The cancer gets into the blood, travels through the blood vessels, and forms a tumor (metastatic tumor) in another part of the body.
The metastatic tumor is the same type of cancer as the primary tumor. For example, if esophageal cancer spreads to the lung, the cancer cells in the lung are actually esophageal cancer cells. The disease is metastatic esophageal cancer, not lung cancer.
The grade of the tumor is also used to describe the cancer and plan treatment
The grade of the tumor describes how abnormal the cancer cells look under a microscope and how quickly the tumor is likely to grow and spread. Grades 1 to 3 are used to describe esophageal cancer:
- In grade 1, the cancer cells look more like normal cells under a microscope and grow and spread more slowly than grade 2 and 3 cancer cells.
- In grade 2, the cancer cells look more abnormal under a microscope and grow and spread more quickly than grade 1 cancer cells.
- In grade 3, the cancer cells look more abnormal under a microscope and grow and spread more quickly than grade 1 and 2 cancer cells.
The following stages are used for squamous cell carcinoma of the esophagus:
Stage 0 (High-grade Dysplasia)
In stage 0, abnormal cells are found in the mucosa or submucosa layer of the esophaguswall. These abnormal cells may become cancer and spread into nearby normal tissue. Stage 0 is also called high-grade dysplasia.
Stage I squamous cell carcinoma of the esophagus
Stage I is divided into Stage IA and Stage IB, depending on where the cancer is found.
- Stage IA: Cancer has formed in the mucosa or submucosa layer of the esophagus wall. The cancer cells are grade 1. Grade 1 cancer cells look more like normal cells under a microscope and grow and spread more slowly than grade 2 and 3 cancer cells.
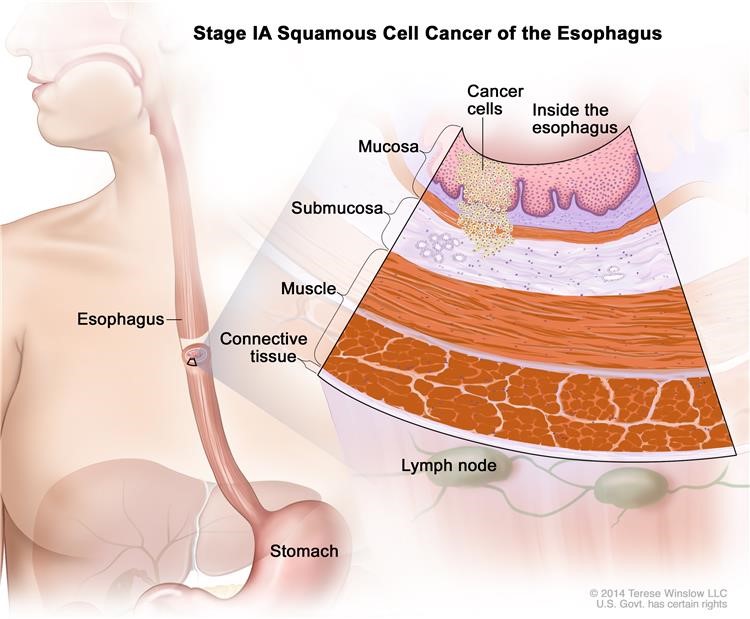
Figure 6: Stage IA squamous cell cancer of the esophagus.
Stage IB: Cancer has formed:
- In the mucosa or submucosa layer of the esophagus wall. The cancer cells are grade 2 and 3; or
- In the mucosa or submucosa layer and spread into the muscle layer or the connective tissue layer of the esophagus wall. The cancer cells are grade 1. The tumor is in the lower esophagus or it is not known where the tumor is.
Grade 1 cancer cells look more like normal cells under a microscope and grow and spread more slowly than grade 2 and 3 cancer cells.
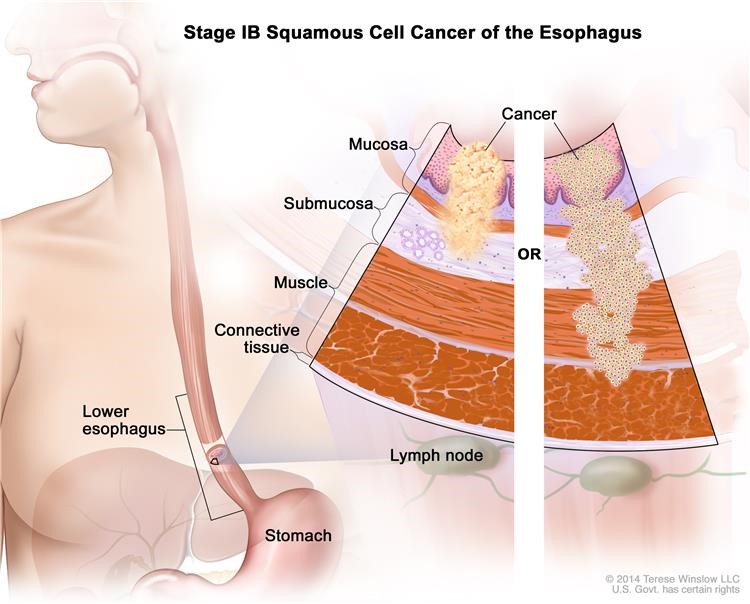
Figure 7: Stage IB squamous cell cancer of the esophagus.
Stage II squamous cell carcinoma of the esophagus
Stage II is divided into Stage IIA and Stage IIB, depending on where the cancer has spread.
Stage IIA: Cancer has spread:
- Into the muscle layer or the connective tissue layer of the esophagus wall. The cancer cells are grade 1. The tumor is in either the upper or middle esophagus; or
- Into the muscle layer or the connective tissue layer of the esophagus wall. The cancer cells are grade 2 and 3. The tumor is in the lower esophagus or it is not known where the tumor is.
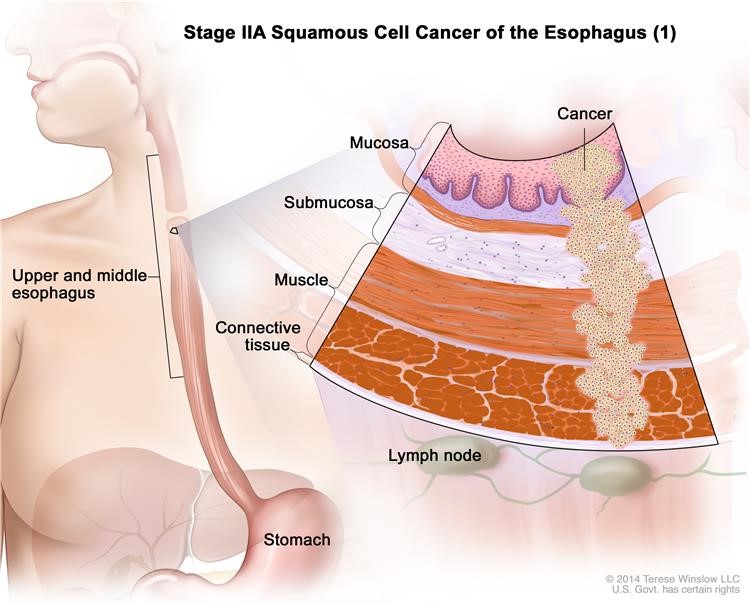
Figure 8: Stage IIA squamous cell cancer of the esophagus (1).
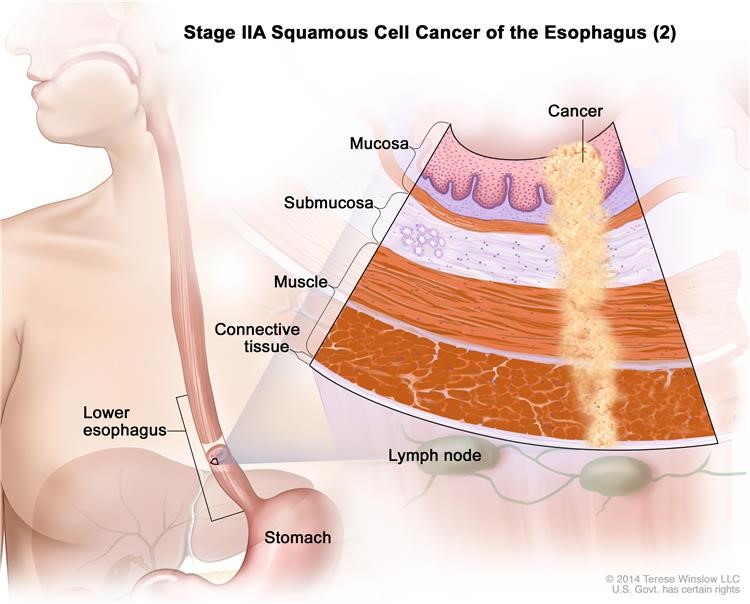
Figure 9: Stage IIA squamous cell cancer of the esophagus (2).
Grade 1 cancer cells look more like normal cells under a microscope and grow and spread more slowly than grade 2 and 3 cancer cells.
Stage IIB: Cancer:
- Has spread into the muscle layer or the connective tissue layer of the esophagus wall. The cancer cells are grade 2 and 3. Grade 2 and 3 cancer cells look more abnormal under a microscope and grow and spread more quickly than grade 1 cancer cells. The tumor is in either the upper or middle esophagus; or
- Is in the mucosa or submucosa layer and may have spread into the muscle layer of the esophagus wall. Cancer is found in 1 or 2 lymph nodes near the tumor.
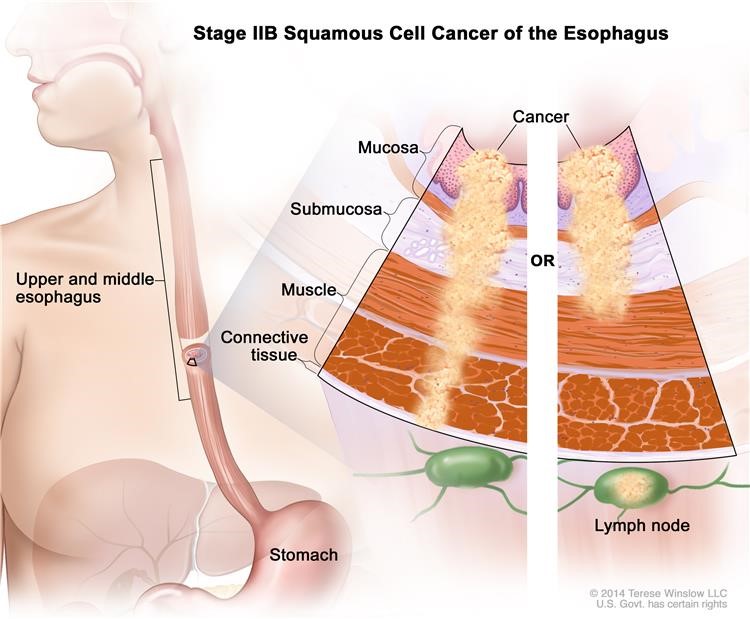
Figure 10: Stage IIB squamous cell cancer of the esophagus.
Stage III squamous cell carcinoma of the esophagus
Stage III is divided into Stage IIIA, Stage IIIB, and Stage IIIC, depending on where the cancer has spread.
Stage IIIA: Cancer:
- Is in the mucosa or submucosa layer and may have spread into the muscle layer of the esophagus wall. Cancer is found in 3 to 6 lymph nodes near the tumor; or
- Has spread into the connective tissue layer of the esophagus wall. Cancer is found in 1 or 2 lymph nodes near the tumor; or
- Has spread into the diaphragm, pleura (tissue that covers the lungs and lines the inner wall of the chest cavity), or sac around the heart. The cancer can be removed by surgery.
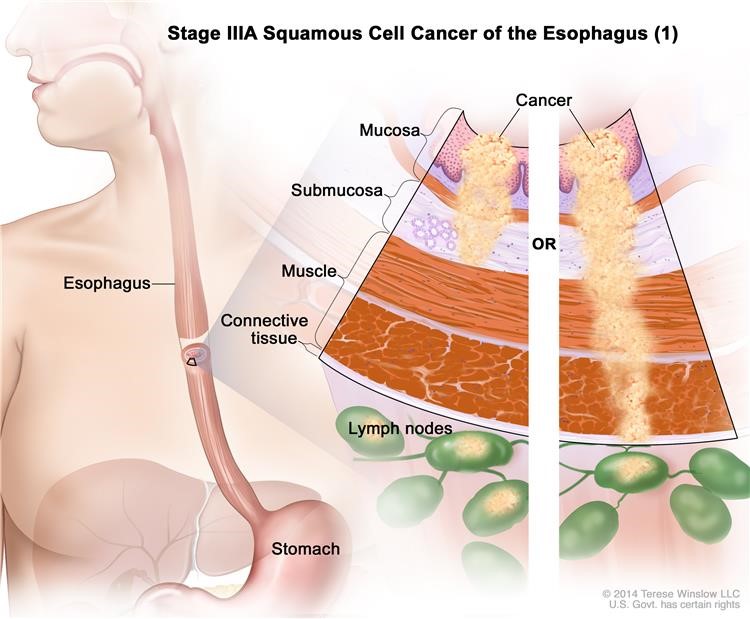
Figure 11: Stage IIIA squamous cell cancer of the esophagus (1).
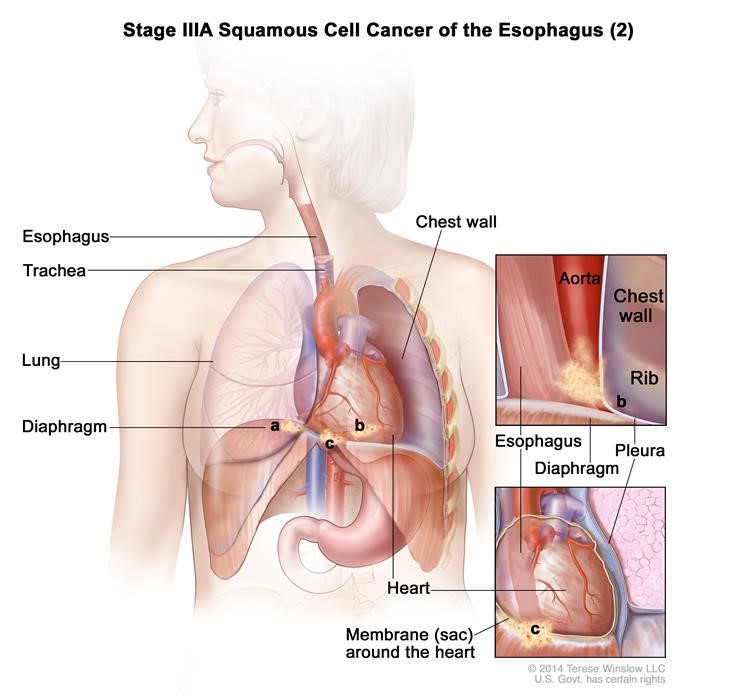
Figure 12: Stage IIIA squamous cell cancer of the esophagus (2).
Stage IIIB: Cancer has spread into the connective tissue layer of the esophagus wall. Cancer is found in 3 to 6 lymph nodes near the tumor.
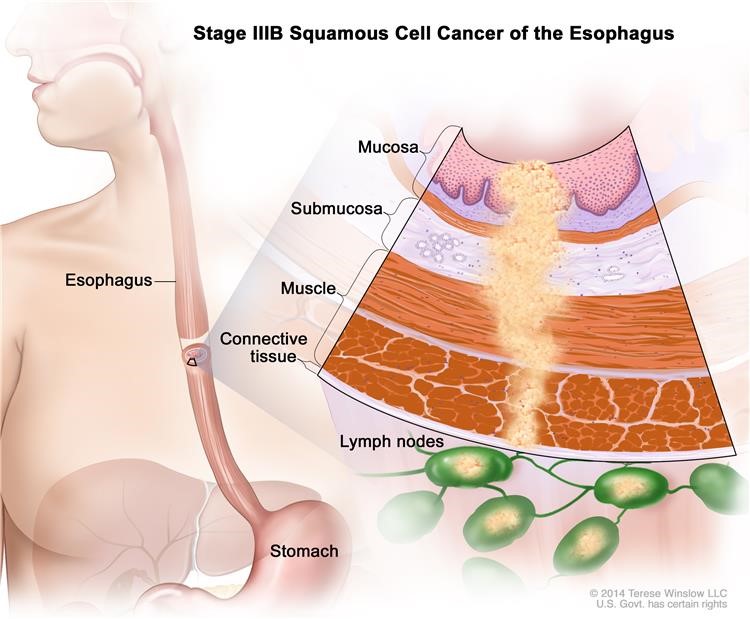
Figure 13: Stage IIIB squamous cell cancer of the esophagus.
Stage IIIC: Cancer has spread:
- Into the diaphragm, pleura (tissue that covers the lungs and lines the inner wall of the chest cavity), or sac around the heart. The cancer can be removed by surgery. Cancer is found in 1 to 6 lymph nodes near the tumor; or
- Into other nearby organs such as the aorta, trachea, or spine, and the cancer cannot be removed by surgery; or
- To 7 or more lymph nodes near the tumor.
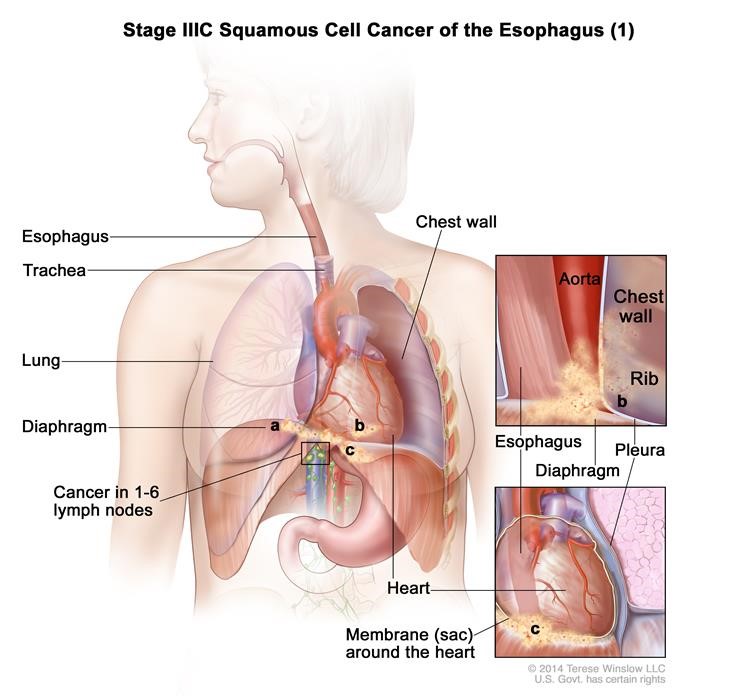
Figure 14: Stage IIIC squamous cell cancer of the esophagus (1).
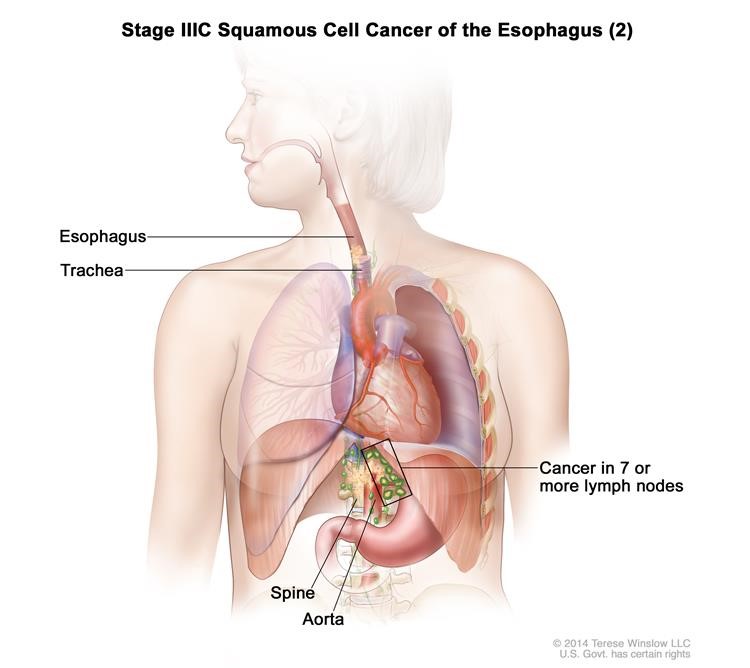
Figure 15: Stage IIIC squamous cell cancer of the esophagus (2).
Stage IV squamous cell carcinoma of the esophagus
In Stage IV, cancer has spread to other parts of the body, such as the lung, liver, adrenal gland, kidney, or bone.
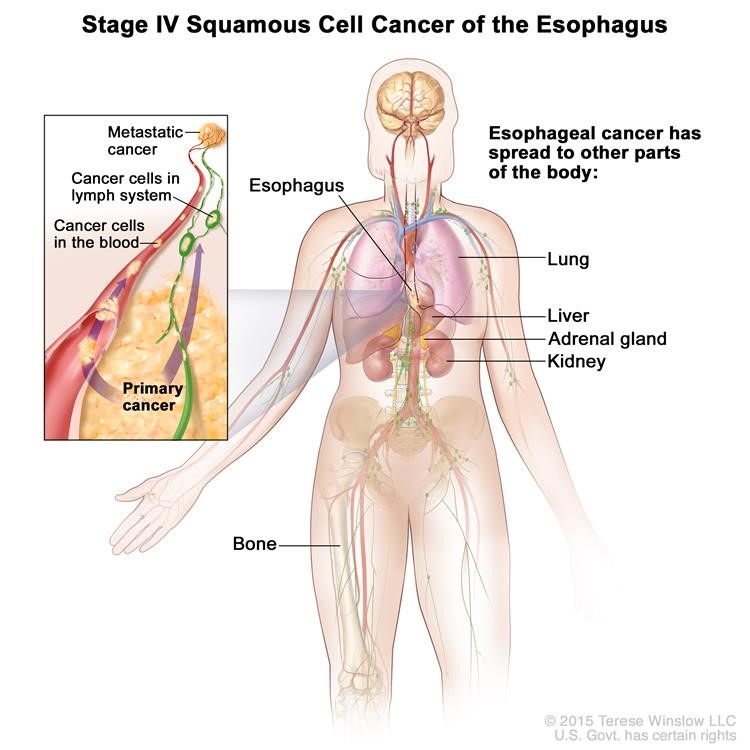
Figure 16: Stage IV squamous cell cancer of the esophagus.
The following stages are used for adenocarcinoma of the esophagus:
Stage 0 (High-grade Dysplasia)
In stage 0, abnormal cells are found in the mucosa or submucosa layer of the esophagus wall. These abnormal cells may become cancer and spread into nearby normal tissue. Stage 0 is also called high-grade dysplasia.
Stage I adenocarcinoma of the esophagus
Stage I is divided into Stage IA and Stage IB, depending on where the cancer is found.
Stage IA: Cancer has formed in the mucosa or submucosa layer of the esophagus wall. The cancer cells are grade 1 or 2. Grade 1 and 2 cancer cells look more like normal cells under a microscope and grow and spread more slowly than grade 3 cancer cells.
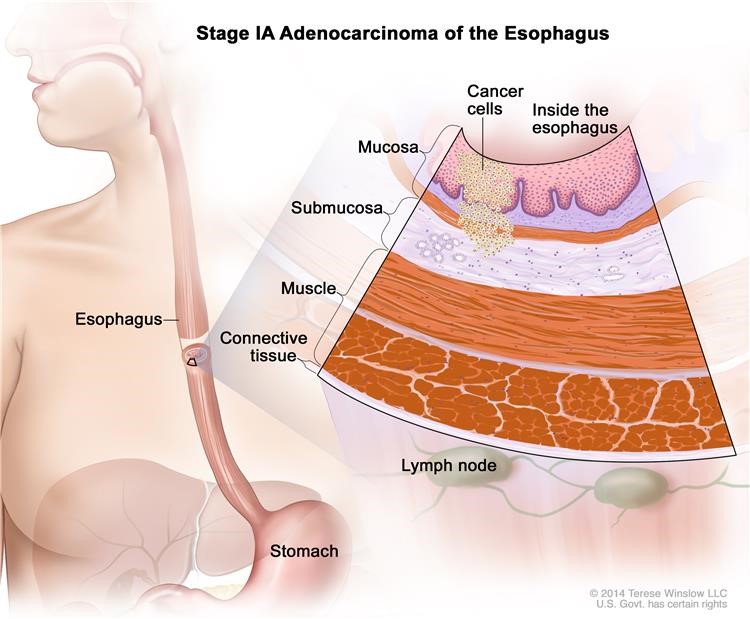
Figure 17: Stage IA adenocarcinoma of the esophagus.
Stage IB: Cancer has formed:
- In the mucosa or submucosa layer of the esophagus wall. The cancer cells are grade 3; or
- In the mucosa or submucosa layer and spread into the muscle layer of the esophagus wall. The cancer cells are grade 1 or 2.
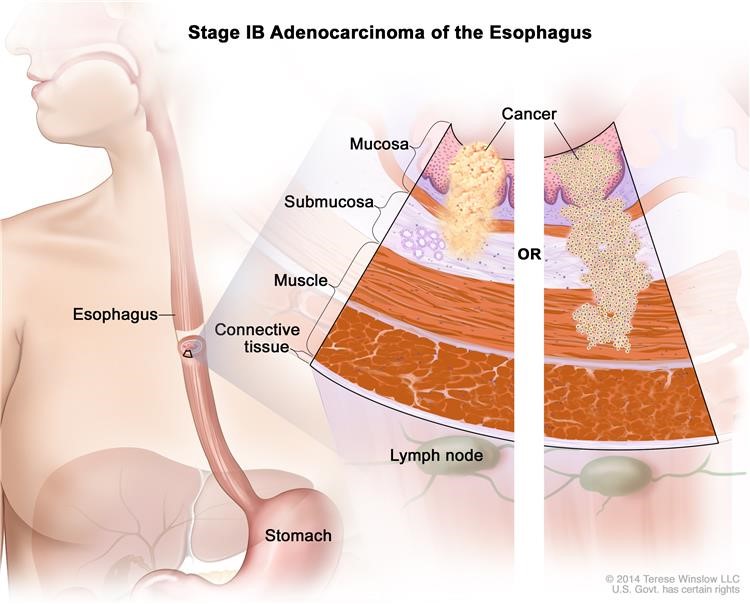
Figure 18: Stage IB adenocarcinoma of the esophagus.
Grade 1 and 2 cancer cells look more like normal cells under a microscope and grow and spread more slowly than grade 3 cancer cells.
Stage II adenocarcinoma of the esophagus
Stage II is divided into Stage IIA and Stage IIB, depending on where the cancer has spread.
Stage IIA:, Cancer has spread into the muscle layer of the esophagus wall. The cancer cells are grade 3. Grade 3 cancer cells look more abnormal under a microscope and grow and spread more quickly than grade 1 and 2 cancer cells.
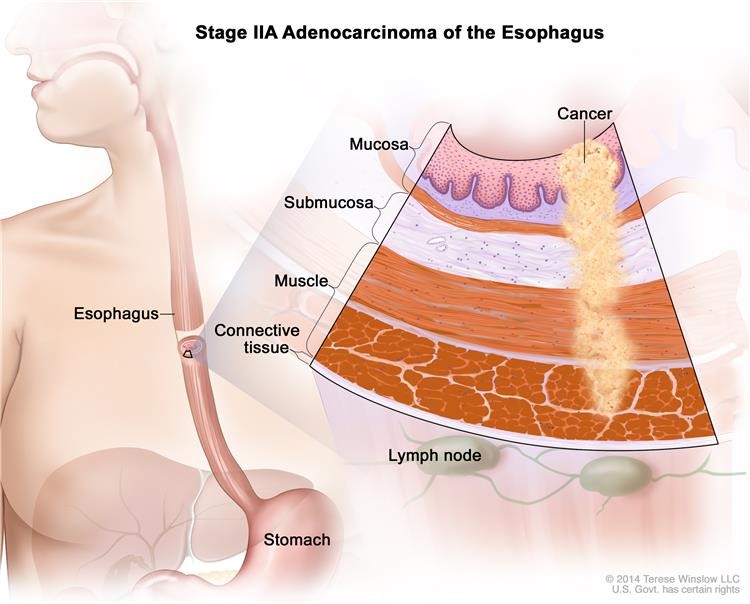
Figure 19: Stage IIA adenocarcinoma of the esophagus.
Stage IIB: Cancer:
- Has spread into the connective tissue layer of the esophagus wall; or
- Is in the mucosa or submucosa layer and may have spread into the muscle layer of the esophagus wall. Cancer is found in 1 or 2 lymph nodes near the tumor.
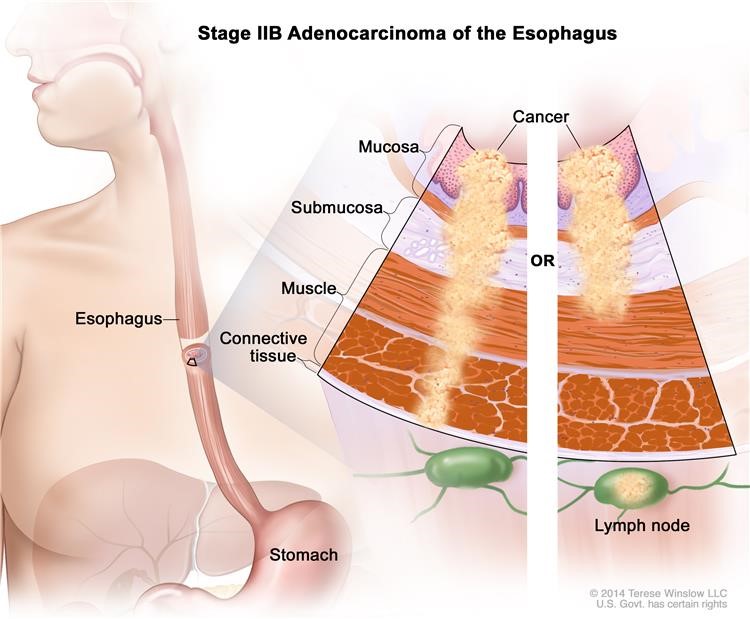
Figure 20: Stage IIB adenocarcinoma of the esophagus.
Stage III adenocarcinoma of the esophagus
Stage III is divided into Stage IIIA, Stage IIIB, and Stage IIIC, depending on where the cancer has spread.
Stage IIIA: Cancer:
- Is in the mucosa or submucosa layer and may have spread into the muscle layer of the esophagus wall. Cancer is found in 3 to 6 lymph nodes near the tumor; or
- Has spread into the connective tissue layer of the esophagus wall. Cancer is found in 1 or 2 lymph nodes near the tumor; or
- Has spread into the diaphragm, pleura (tissue that covers the lungs and lines the inner wall of the chest cavity), or sac around the heart. The cancer can be removed by surgery.
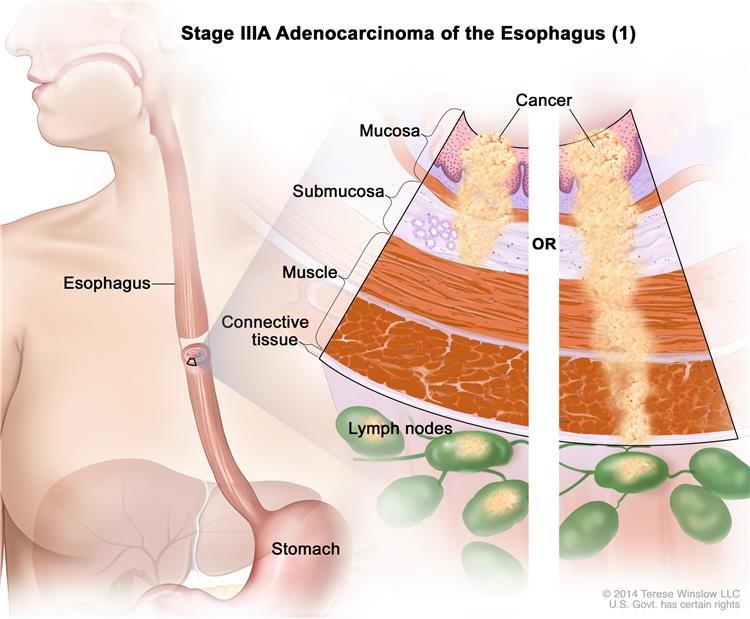
Figure 21: Stage IIIA adenocarcinoma of the esophagus (1).
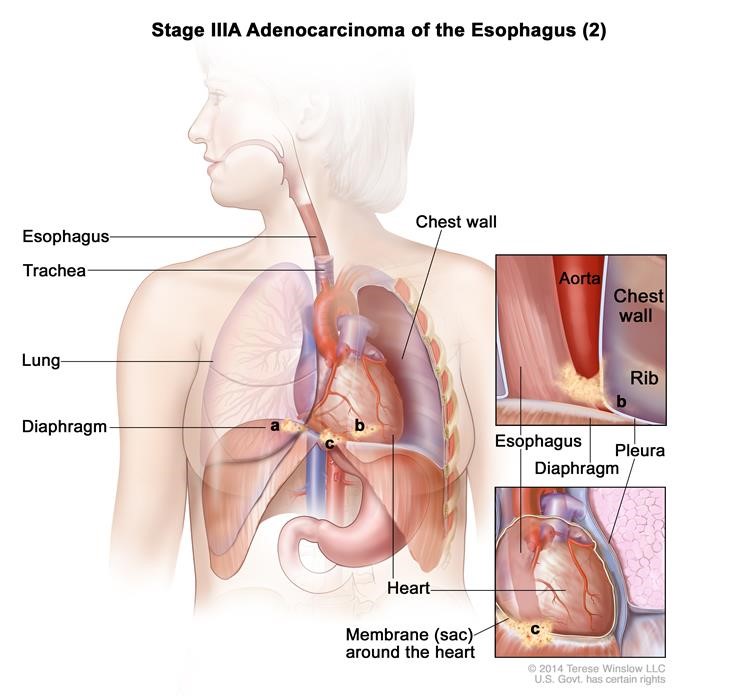
Figure 22: Stage IIIA adenocarcinoma of the esophagus (2).
Stage IIIB: Cancer has spread into the connective tissue layer of the esophagus wall. Cancer is found in 3 to 6 lymph nodes near the tumor.
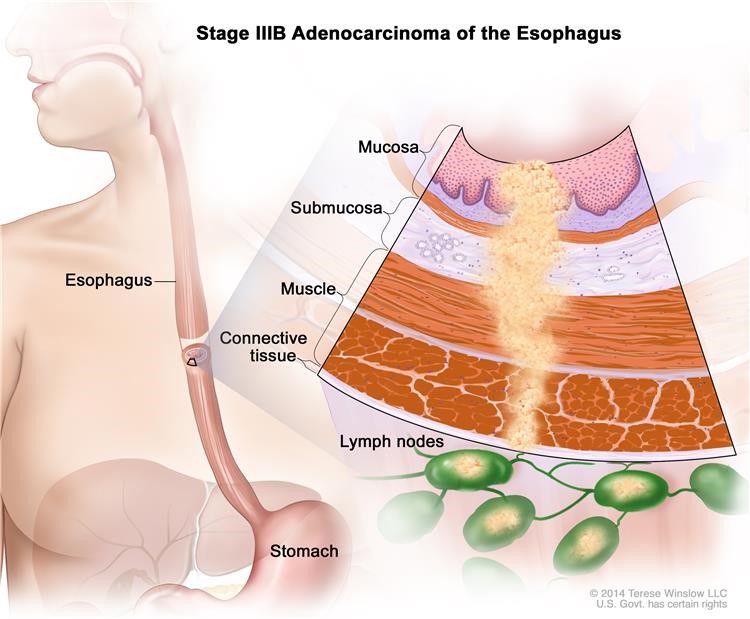
Figure 23: Stage IIIB adenocarcinoma of the esophagus.
Stage IIIC: Cancer has spread:
- Into the diaphragm, pleura (tissue that covers the lungs and lines the inner wall of the chest cavity), or sac around the heart. The cancer can be removed by surgery. Cancer is found in 1 to 6 lymph nodes near the tumor; or
- Into other nearby organs such as the aorta, trachea, or spine, and the cancer cannot be removed by surgery; or
- To 7 or more lymph nodes near the tumor.
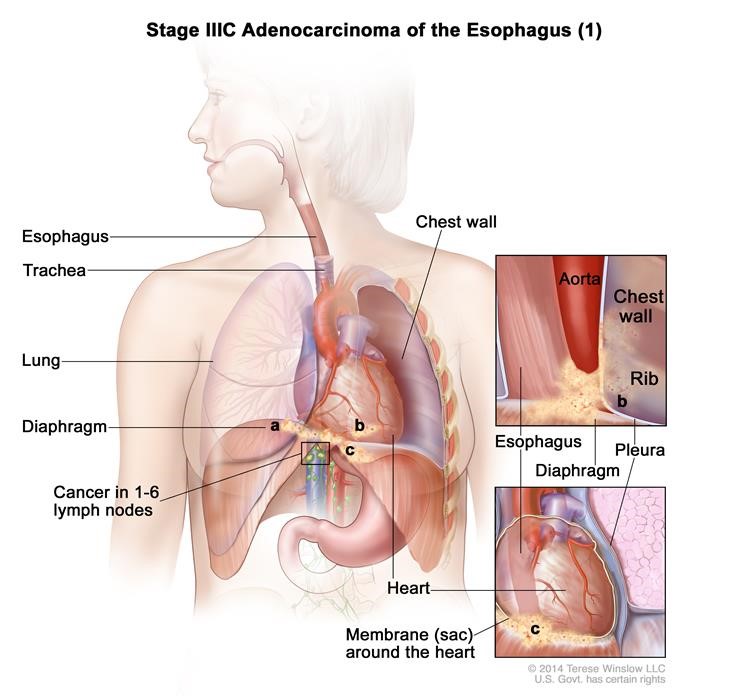
Figure 24: Stage IIIC adenocarcinoma of the esophagus (1).
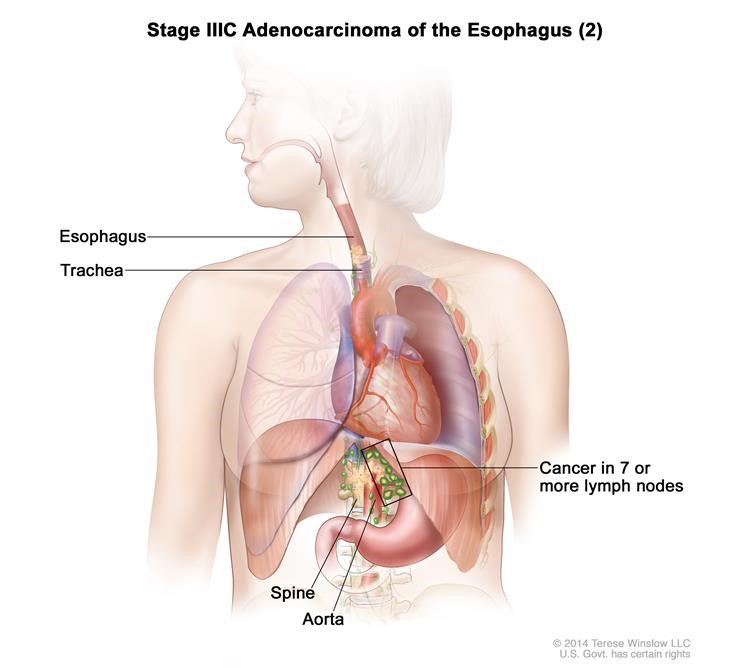
Figure 25: Stage IIIC adenocarcinoma of the esophagus (2).
Stage IV adenocarcinoma of the esophagus
In Stage IV, cancer has spread to other parts of the body, such as the lung, liver, adrenal gland, kidney, bone.
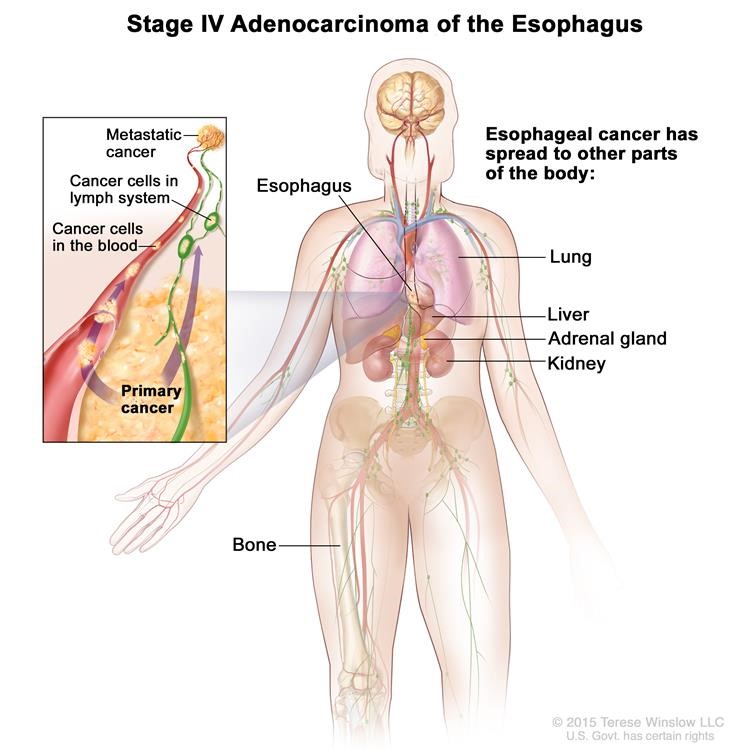
Figure 26: Stage IV adenocarcinoma of the esophagus.
Meeting With Your Surgeon
After these tests are completed, the thoracic surgeon will have a discussion with you about whether surgical repair is recommended.
If both you and the thoracic surgeon agree to proceed with surgery, the operation date will be booked.
This is a great opportunity to ask as many questions as you want.
After Your Surgery (Post-Op)
How Long Will I Stay in Hospital?
After your surgery, you will stay one night in the Critical Care Unit (CCU), and then stay in a regular hospital room for a week after your surgery.
How Will I Feel Post-Op?
After your surgery, you will have to make a number of adjustments to daily life, including changes to your eating and sleeping habits.
Immediately after surgery, you will have a feeding tube in your belly. After a period of time, you will be able to eat normally, and the tube will be removed. This usually happens around 4-6 weeks post-op.
NEED: OSLER DIETARY GUIDELINES – SAME AS HIATUS HERNIA REPAIR?
Since your stomach will be significantly smaller post-op, you will benefit by eating smaller meals than previously, and more frequently.
Normal Symptoms After an Esophagectomy:
Contact Your Surgeon if You:
- Have new redness or swelling around your incisions
- Have leaking fluid (drainage) or pus from an incision
- Feel more pain than usual around an incision
- Have a fever (temperature higher than 38.5 °C or 101 °F)
What Kind of Activity Can I Do?
At the Hospital
The evening of your surgery, we will have you sitting in a chair and walking in the hallway. Being active reduces the risk of blood clots, and improves your breathing to prevent pneumonia.
The nursing staff on the surgical ward will insist on getting you out of bed!
At Home
While you should avoid strenuous activities during your recover, specific activities are recommended to promote a complete return to health and mobility.
Below are instructions on activity post-op:
|
Household Activities: After discharge from the hospital, avoid lifting more than 15 pounds for at least 4 weeks, and avoid excessive bending or twisting for 2 weeks following surgery. We also suggest you avoid household activities like vacuuming, carrying groceries, or shoveling snow for at least 4 weeks. Every time you lift or push heavy objects, you strain the hiatus. Although this usually isn’t a problem, repeated force may undo all the work that was done. We do encourage you to walk every day to regain your strength after surgery |
|
|
Driving: Avoid driving until you no longer need narcotic pain medication and you feel you can make rapid movements unimpaired by pain. Driving while taking narcotics can impair your ability to drive safely. |
|
|
Work: You should be able to return to work in X weeks. If your job involves heavy lifting and light duty is not an option, you may need up to X weeks off work to recover. |
|
|
Sports: We suggest avoiding sports for 4 weeks. You can go for brisk walks 10 days after surgery. Wait 2 weeks before you swim. |
Taking Care of Your Incisions
When Can I Remove the Dressings?
After a minimally invasive esophagectomy, small white dressings are typically placed over each incision. These dressings may be removed 48 hours (2 days) after the operation.
Below this dressing are small brown or white pieces of tape (called Steri-Strips™); these will fall off on their own within 1-2 weeks. If they don’t fall off, you can remove them in the shower after two weeks.
If your surgeon gives you specific instructions other than this, please follow those instructions.
BathingYou can shower 48 hours after the surgery (after the gauze and clear tape dressing is removed). It is okay to get soap and water on the incisions. Pat the area dry. We recommend that you don’t submerge yourself in water (in a bathtub, pool, or hot-tub) for at least two weeks post-op. |
When to Contact Your Doctor
If you notice drainage from your incisions, particularly if it is thick and foul-smelling or associated with a fever, contact your surgeon immediately.
If you notice redness around your incisions, especially if it is getting worse or associated with drainage or a fever, contact your surgeon.
Pain Management and Medication
Although your surgery was likely completed using keyhole incisions you may have some pain. You will be given a PCA, a patient controlled analgesia, which allows you to press a button for additional medication when you need it.
At Osler we have an “Acute Pain Service” that is supervised by an anesthesiologist and a nurse practitioner. They will see you a few times to make sure you are comfortable.
Your pain should be controlled well enough for you to begin getting out of bed the morning after surgery.
You will be discharged with pain medication, typically a mild to moderate strength narcotic. Take as needed and as prescribed.
Other Medications
You will be prescribed a stool softener when you go home. Narcotic or pain medications can cause constipation and a stool softener may help. If you have some nausea at home, you can pick up some Gravol® from the pharmacy.
Your Regular Medications
Unless otherwise instructed, continue to take your usual home medications once you are home.
Follow-Up
You will be given a date and time to see your surgeon following surgery, usually in 3 weeks.
The follow-up appointment should have been arranged during the office visit. If not, please call 905-458-4520 to arrange an appointment.