Your Osler Journey is to be used for informational purposes only. It is not a substitute for medical advice. You should always consult a doctor if you have any questions regarding the information set out in the "Journey".
The Osler Thoracic Diagnostic assessment program
The Thoracic Diagnostic Assessment Program (DAP) has a rich history of cutting-edge care for patients with lung and esophageal cancer. Physicians from Osler perform 95% of all lung and esophageal surgeries using a minimally invasive approach, and have taught these techniques to other surgeons thoughout Canada. A minimally-invasive approach means a faster recovery, with less post-operative pain.
Patient-centered care is our number-one priority. Our goal is to maintain and improve your quality of care by making the process of diagnosis and treatment more efficient and supportive. We reduce your number of visits, we clarify each step of your care experience, and we provide you and your families information on demand. We do our best to help make this process as transparent as possible, and to support patients and their families through this difficult time.
Our DAP accepts referrals from any physician who has a patient that presents with a suspicious Chest X-ray or CT scan.
Your Osler Journey
"Your Osler Journey" is a unique way for you to learn about what to expect as you move through the Lung Cancer Treatment Pathway at Osler.
Here we take you through the very personal experience of Mr. Paul Ross:
Paul's case represents his journey through lung cancer. Everyone's case is unique. You may require more or different visits than Paul, and you may go through some different tests.
This information is not intended to contradict or replace your physician's advice or personalized treatment plan for you. It is meant to serve as a reference for terms, tests, and steps you may encounter on your own journey.
You should ultimately consult your own physician on the specific steps in your journey.

Paul is a 65 year old married gentleman. He is a father of one son, and recently became a grandfather! He is healthy, besides being a smoker for 30 years. He tried quitting many times, but was never completely able to stop smoking.
This virtual timeline will guide you through Paul's experience. His experience is typical of what most patients within our Lung Cancer DAP can expect.
Paul's timeline can be divided into key visits, with the first visit being the day he talks to his family doctor about some concerning symptoms he's been having: Day 1.
Clinical Suspicion
Paul had a nasty cold that just wouldn't completely go away. He had a nagging cough that wouldn't get better, and chest pain, so he went to see his family doctor, Dr. Manson Mak.
Paul explained how he was feeling to Dr. Mak, and Dr. Mak ordered a CT scan of Paul's chest. Dr. Mak also counselled Paul on how important it is to quit smoking.
REFERRAL FOR A CT SCAN AT WILLIAM OSLER HEALTH SYSTEM
Paul got a call from the Diagnostic Imaging Department at William Osler Health System.
He had his appointment booked at Brampton Civic Hospital. He answered a few questions about his allergies, medications, and other medical problems.
Unlike many centres in the GTA, Osler is blessed with 12 CT scanners that allow us to minimize wait times. If requested urgently, a CT scan can be completed in 5 days.
Enter through main entrance facing Bovaird Drive.
Turn left at the elevators.
The Diagnostic Imaging (DI) department is located on the 1st floor in the main atrium. Register at the desk, and we will take care of the rest!
Enter hospital through the main entrance.
Follow signs to Diagnostic Imaging, located on the main level.

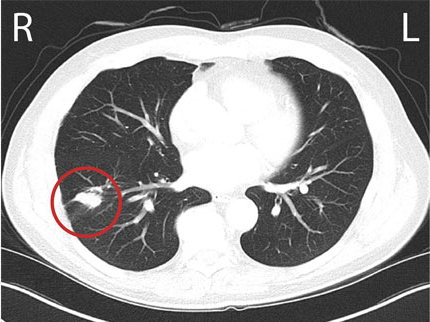
A chest CT scan is similar to but much more detailed than a chest X-ray image. It allows doctors to have an accurate image of your lungs, heart, esophagus and lymph nodes.
CT stands for Computed Tomography. This painless imaging test takes many detailed X-ray images, called slices, of your lungs and the inside of your chest. Computer software combines these slices to create three-dimensional (3D) models to help show the size, shape, and position of your lungs and structures in your chest.
A chest CT scan can help doctors look for:
- Excess fluid around the lungs that is known as pleural effusion
- Clots in the lung (pulmonary embolism)
- The location and size of any tumour in the lung
- Any enlarged lymph nodes
- Infections of the lung
During the CT scan
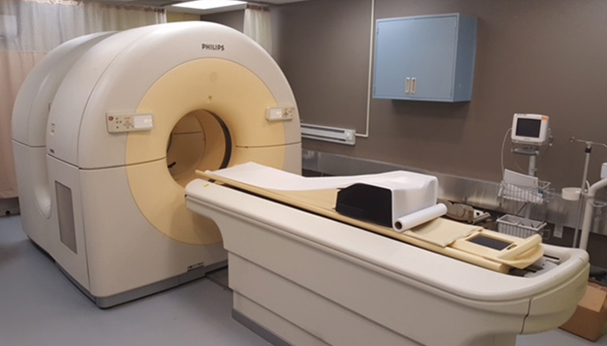
Our CT scanner is a large, tunnel-like machine that has a table. You will lie still on the table and the table will slide into the scanner.
It is not as tight as an MRI machine. If you are very claustrophobic, your family doctor may give you medicine to relax you during the test.
You will hear soft buzzing or clicking while you are inside the scanner and the scanner is taking pictures. You will be able to hear and talk to the technician performing the test while you are inside the scanner.
The technician will ask you to hold your breath for a short part of the test. This is important because it will prevent the normal breathing movements, and you need to be still to take clear X-ray images.
We often inject a dye into a vein in your arm before the CT scan. This contrast dye highlights blood vessels inside your chest and creates much clearer images. You may feel some discomfort from the needle. After the dye is injected, you may also briefly feel warm or have a temporary metallic taste in your mouth.
After the CT scan
After a CT scan involving an iodine-based dye (contrast), it is a good idea to increase your fluid intake to help remove the contrast from your body more quickly.
What are the risks of a CT scan?
Chest CTs are very safe, but there are a few risks you should know about:
- Allergic reaction to the contrast dye: It is very important to tell your doctor and the radiation technician if you have any allergies or have had a previous reaction to dye. If you are determined to be high risk for a reaction, you can be premedicated to prevent it. Breastfeeding patients may have to "pump and dump" for 2-3 days after a contrast enhanced CT.
- Slight risk of cancer: This risk is particularly in growing children, because the test uses X-ray images, which are a form of radiation. The radiation from one CT scan is similar to the radiation you would get from your environment accumulated over three years. This is only a concern if you receive multiple CT scans over your lifetime. A CT scan should be avoided in pregnant women.
- Detection of unrelated abnormalities: Another risk is that the chest CT scan may detect something unrelated to the reason why you had the scan ordered. This may be something that doesn't cause any symptoms now, but may require more tests once it is discovered.
Paul's CT scan detected a 2.5 cm nodule in the lower lobe of his right lung.

Dr. Mak saw this report and immediately faxed a referral to Osler's Thoracic Diagnostic Assessment Program (DAP).
Referral to Osler's Thoracic DAP

Paul received a phone call 24 hours after Dr. Mak faxed the referral to Osler's Thoracic DAP. The call was from our Nurse Navigator, Juliett Phinn.
Paul expressed his anxiety about his potential diagnosis. Juliett was very reassuring and comforting. She promised to do everything she could to make this journey seamless and well-informed. She asked Paul about his medical history, and asked him for more information about his current illness.
She scheduled an urgent appointment with the thoracic surgeon at Osler's DAP.
We know that a patient may feel an overwhelming number of emotions when their family doctor tells them they may have lung cancer.
At the heart of our Thoracic DAP at Osler is our Nurse Navigator, Juliett Phinn. She is there to help make your patient journey as seamless as possible. Her role is to compassionately guide you and your family through this process, and she can help you by:
- Making sure you as a patient have a firm schedule of accurate appointment times
- Making sure you have the transport you need to these appointments
- Helping you and your family interpret complex test results
- Inform you and your family of all your options
- Provide any support you may need through this process
Our Thoracic Nurse Navigator is available throughout the day by email or telephone to answer questions, provide support, and make sure the patient is receiving timely care.
Patients and their families may access Nurse Navigator services as often as needed.
Juliett can be reached at:
juliett@oslerhealth.ca
and at:
905-123-4567
APPOINTMENT WITH THORACIC SURGEON
Paul lives in Brampton, so he requested to be seen at the Springdale Medical Centre, and was scheduled for 10 am.
We appreciate that travelling in the GTA can be challenging. Once your family doctor has decided to refer you to our clinic, you can ask our Navigator to book the appointment in one of our three clinics:
Springdale Medical Centre
Brampton Civic Hospital: Thoracic Surgery Clinic
Etobicoke General Hospital
During this meeting you will meet our surgeons:

Paul arrived with his wife on time and was greeted by our staff: Selma and Raman. He also met our Nurse Navigator for the first time. His thoracic surgeon, Dr. Kashif Irshad, invited the couple into his office.
image missing
Our staff at Springdale Medical Centre, Selma (left) and Raman (right), and our Nurse Navigator Juliett (center).
Dr. Irshad and Paul had a comprehensive discussion about the possibility of this lung nodule being a lung cancer.
Dr. Irshad explained that based on the initial CT scan, the lung nodule most likely represents a Stage 1 non-small cell lung cancer.
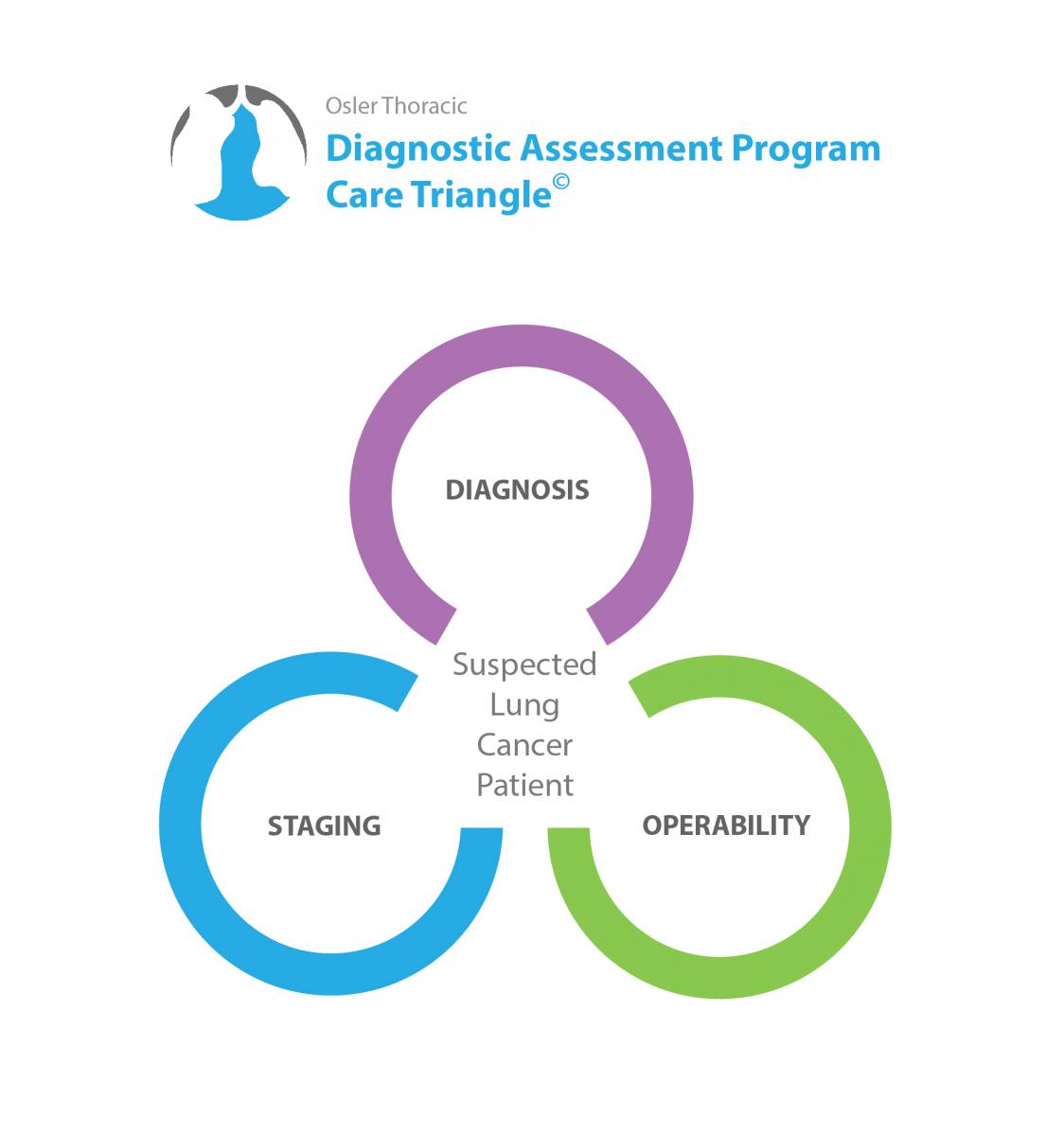
Dr. Irshad went over Osler's Thoracic-DAP Care Triangle©, and made some recommendations on how to confirm the diagnosis, stage the cancer, and assess whether Paul would be strong enough for lung surgery (assess his operability).
Every test we do is meant to gather information around 3 key components in your care: Diagnosis, Staging, and Operability
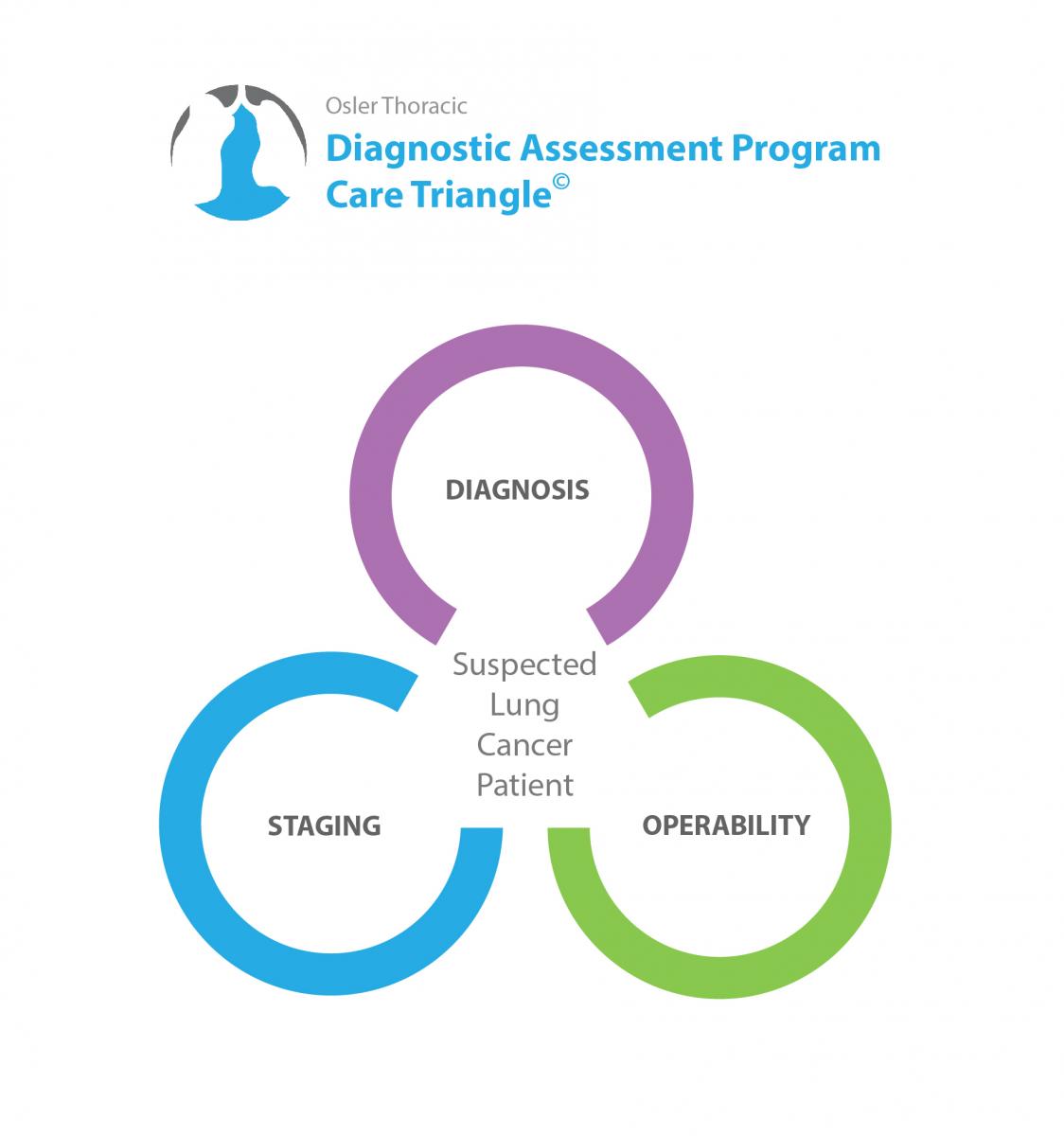
Osler Thoracic-DAP Care Triangle©
Confirming the diagnosis: These tests are aimed at confirming or disproving a lung cancer diagnosis.
In patients where lung cancer is the likely diagnosis, we will order tests to help with staging. The stage of the cancer often determines the course of treatment we will pursue.
Your surgeon may order tests to evaluate your overall health, and your ability to tolerate surgery. These tests will examine your operability.
Diagnostic and Staging Tests Ordered
After the discussion, Paul agreed to undergo a more extensive workup. Dr. Irshad ordered, a CT-Guided needle biopsy to make a diagnosis, a PET scan and brain MRI for staging, and Pulmonary Function Tests to assess his operability.
In a needle biopsy, a needle is used to take a small sample of the lung tumour for testing.
Before the needle biopsy
Most needle biopsy procedures don't require any preparation on your part. However, you may be asked to stop taking blood-thinning medications, such as warfarin (Coumadin) or aspirin, in the days before your biopsy. Your doctor may ask you not to eat or drink 6-8 hours before the procedure.
Another CT scan is usually done before your needle biopsy to reassess the lesion and to plan the approach.
During the needle biopsy
A special type of radiologist, called an interventional radiologist, will perform your biopsy. They will position you in a way that makes it easy to access the area where the needle will be inserted. You may be asked to lie on your back, side or stomach.
After cleaning and numbing the skin where the needle will be inserted, the doctor will guide a needle through your skin and into the area of interest. A small sample is collected and the needle is withdrawn. This process may be repeated several times until enough of a sample is collected.
The biopsy can be done with a smaller needle (a fine needle aspirate) or a larger needle (core needle biopsy) depending on how large of a sample is needed. Often, the radiologist uses a chest CT scan or special x-ray machine called a fluoroscope to guide the needle.
The specimen will be placed in a container that contains formalin to preserve the structure of the cells within the sample. The container is immediately sent to the Department of Laboratory Medicine at William Osler Health System.
What are the risks of a needle lung biopsy?
- Pneumothorax: A partial collapse of the lung after the biopsy occurs in about 20% of patients. If this happens, you would need to be observed with a repeat X-ray for a few hours. Most can be managed without treatment, but a few require a small tube to be placed to re-expand the lung
- Bleeding in the lung occurs in about 10% of patients. Occasionally, the patient may cough up small amounts of blood after the biopsy.
The specimen will be processed and placed on slides for our Pathologists to review. At Osler we are blessed with an exceptional group of pathologists who have a unique expertise in the diagnosis of lung cancer.
A PET/CT scan is a nuclear medicine imaging test that uses a mild form of radioactive sugar to find areas in the body that are metabolically active. PET imaging can be fused with a regular CT scan to allow radiologists to better see the areas that are hypermetabolic, or more active than the body's base metabolism or activity.
Every cell in the body consumes glucose (sugar) to survive. Cancer cells are often more active than normal body cells, and so they take up and consume more glucose.
The PET scanner is made up of many detectors that detect the radioactive sugar in the body. A computer analyzes the patterns of radioactivity and creates 3-dimensional colour images of the area being scanned. Different colours on a PET image represent different levels of activity between the body structures.
There are 3 items that your thoracic surgeon will look at when reviewing a PET/CT scan:
- Is the main lung tumour metabolically active? When a lung lesion is active, this may mean there are cancer cells present. However, there are some causes for increases in PET activity that are not caused by cancer.
- Has cancer spread to the surrounding lymph nodes? If there is activity in the lymph nodes close to the lung, there is a higher chance that they may have cancer cells within them. This might mean a more advanced cancer stage.
- Has the cancer spread anywhere else in the body? A PET/CT scan examines the entire body except the brain. This makes it a very useful tool to be sure the cancer hasn't spread anywhere else.
It is important to remember that PET/CT cannot confirm whether cancer cells are or are not present. Your thoracic surgeon will talk about the considerations and limitations of this test with you during your follow up appointment.
Only 82% of lung cancer nodules or lesions are active on PET/CT. There are many cancers that don't take up much sugar, and there are many benign nodules or lesions that do take up sugar.
40% of lymph nodes that are active on PET scan don't have cancer cells. Therefore, even if the PET scan suggests cancer may have spread to the lymph node, a biopsy must be taken to confirm this.
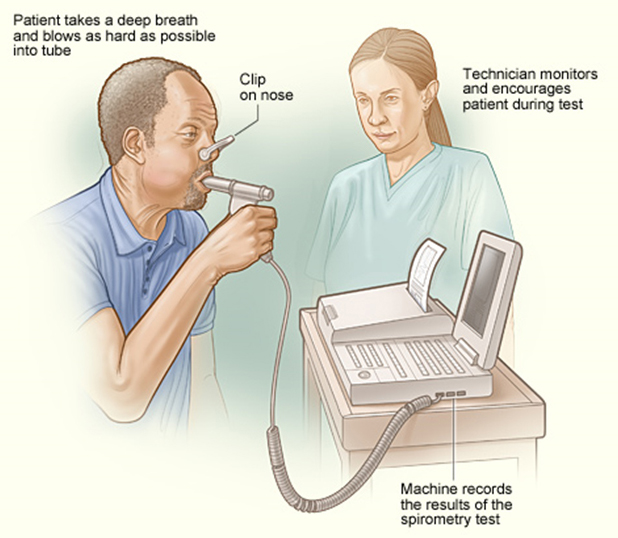
A pulmonary function test is a non-invasive test that measure how well the lungs work. It measures how much air the lungs can take in and expel, and how quickly and efficiently they do this. The most common type of pulmonary function test is spirometry, and another is called plethysmography.
Spirometry
During a spirometry test, you will be asked to breathe into a long tube with a sterile mouthpiece. A clip will be placed on your nose so that you are only breathing through your mouth. A techician or respiratory therapist will guide you through the test, and takes a variety of measures.
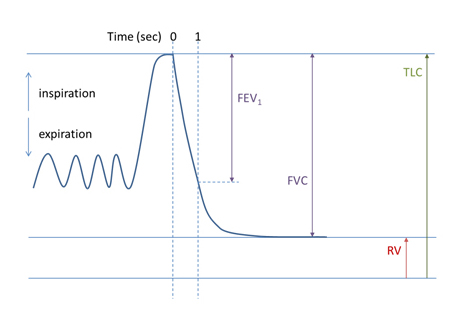
The measurements of a spirometry test may be visualized onto a graph called a pneumotachograph, shown below:
Plethysmography
During this test, you are asked to sit or stand in an airtight glass booth. The technician or respiratory therapist will ask you to blow into a tube connected to the plethysmograph, which will measure your lung function by monitoring changes in the air volume and air pressure within the booth.
What are the risks of a pulmonary function test?
For healthy individuals, this is a very low risk. However, you may experience the following:
- Dizziness/lightheadedness: Since this test will require you to breathe in and out quickly and deeply, you may become lightheaded or faint. If you feel lightheaded at any time, tell your technician / respiratory therapist
- If you have asthma: the deep breating involved for the test may trigger an asthma attack.
DIAGNOSIS
Diagnostic tests such as a bronchoscopy, needle biopsy, endobronchial ultrasound, or mediastinoscopy are essential in the Diagnosis stage of the Osler Thoracic-DAP Care Triangle
Your bronchoscopy will be performed by your thoracic surgeon.
In this test, the doctor passes a thin, flexible tube with a light on the end into the mouth or nose, and down into the breathing passages of the lungs. The tube lets the doctor see inside the lungs. Tiny tools inside the tube can take samples of fluid or tissue so the pathologist can examine them.
Patients are given mild anesthesia or sedation during a bronchoscopy. Most patients usually wake up not remembering the procedure at all.
Before the bronchoscopy
You'll need to avoid eating or drinking anything for 8 hours before the bronchoscopy. Before the procedure, ask your surgeon if you need to stop taking:
- Aspirin
- Ibuprofen
- Warfarin
- Other blood thinners
Bring someone with you to your appointment or arrange for transportation home after.
Remember: we won't be able to give you sedation if you don't have someone reliable to take you home.
During the bronchoscopy
Once you're relaxed, your surgeon will insert the scope into your mouth. The bronchoscope will be passed down your throat until it reaches your bronchi, the airways in your lungs.
Your doctor may wash your lungs by sending a warm saline solution through the bronchoscope, and then removing it. Cleaning your airways makes examination easier and gives your doctor samples of your lung cells, and of what they produce. The doctor may attach a brush or needle to the bronchoscope to collect samples from your lungs. These samples can help your surgeon diagnose what was found on your CT scan.
Ultrasound is a type of test that uses sound waves to create pictures of the inside of your body. A small, microphone-like instrument called a transducer gives off sound waves and picks up the echoes as they bounce off different body tissues. The echoes that are sent back to the transducer are converted by a computer into an image on a computer screen.
The thoracic surgeon can interpret ultrasound images and decide if the structures look normal, or if a biopsy is necessary.
Before the endobronchial ultrasound
Before an endobronchial ultrasound, you may be given a numbing medicine (local anesthesia) and light sedation, or you may be put under general anesthesia.
During the endobronchial ultrasound
A bronchoscope is fitted with an ultrasound transducer at its tip. It is passed through your mouth, and down into your windpipe.
The transducer can be pointed in different directions to look at lymph nodes and other structures in the mediastinum (the area between your lungs).If the doctor sees any suspicious areas, such as enlarged lymph nodes, the doctor can take a sample of these areas using a needle passed through the bronchoscope.

Bronchoscope obtaining lymph node biopsy
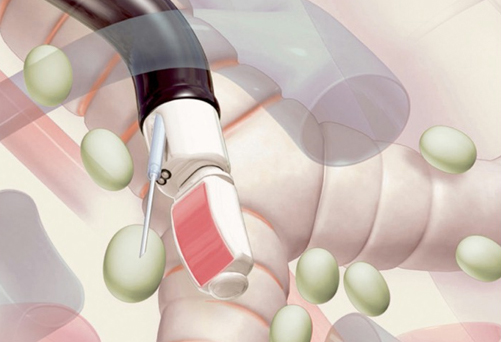
Ultrasound guides lymph node biopsy
The samples are then sent to our pathologist to look at under the microscope.
Paul presented to the Department of Diagnostic Imaging at the Brampton Civic Hospital.
He met Dr. Leslie Vanderberg, one of the interventional radiologists. After freezing the skin on his chest, Dr. Vanderberg guided a small needle into Paul's tumour to take a biopsy specimen for analysis.
The specimen was immediately sent to the lab for analysis by the pathology team.
Pathologists are doctors who specialize in studying cells and tissue samples for signs of disease. Once they receive the sample or biopsy, they examine the cells of the tissue to make a diagnosis.Pathologists create a pathology report for the surgeon. Once your doctor receives the report, our Nurse Navigator will contact you to set up a follow-up appointment with your surgeon.

Dr. Syed Ismael, a top lung pathologist
You can request a copy of your pathology report from your doctor. Pathology reports are usually filled with technical terms, so you may find it helpful to have your doctor review the report with you.
Your pathology report may include:
- A description of the biopsy sample: This section of the pathology report, sometimes called the gross description, describes the biopsy sample in general. For example, it may describe the colour and consistency of the tissues or fluid collected by the needle biopsy procedure. Or it may say how many slides were submitted for laboratory analysis.
- A description of the cells: This section of the pathology report describes how the cells appear under a microscope. This section may include how many cells and what types of cells were seen. Information on special dyes that were used to study the cells in order to gather more information about the diagnosis and the best treatments also may be included.
- The pathologist's diagnosis: This section of the pathology report lists the pathologist's diagnosis. It may also include comments, such as whether other tests are recommended.
If the specimen has cancerous cells, the pathologist will tell us which type it is.
There are 2 main types of lung cancer: small cell cancer, and non-small cell cancer. They are described below.
Small Cell Cancer
Small cell lung cancer accounts for 10%-15% of all lung cancers. It usually starts in the bronchi in the centre of the lungs. Small cell lung cancer is the most aggressive of all types of lung cancer. In many cases, it has spread to other parts of the body by the time it is diagnosed. Small cell lung cancer is named so because the cells look very small when examined under a microscope.
Non-Small Cell
Non-small cell lung cancer is the most common type of lung cancer. It is the type most commonly found in women, non-smokers, and young adults.
It does not spread as quickly as small cell lung cancer but is still often diagnosed when it is at an advanced stage. It's important to note that even though an advanced non-small cell lung cancer is inoperable, it is still treatable. There have been many recent advances in the treatment of lung cancer, and survival rates are improving for all stages of the disease.
It is surprising to many that people who have never smoked can and do develop lung cancer. In fact, the majority of people who develop non-small cell lung cancer today are non-smokers: they are either former smokers or have never smoked.
One in five women who develop lung cancer have never smoked. And while lung cancer is decreasing in older people and in men, it is increasing in young adults, especially young women who have never smoked.
There are 3 primary types of non-small cell lung cancer. These include:
Adenocarcinoma
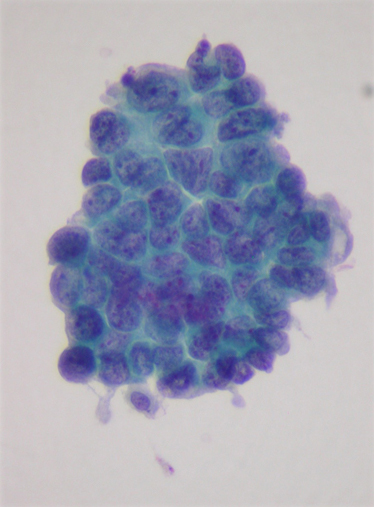
Adenocarcinoma is the most common type of non-small cell lung cancer. It accounts for up to 50% of cases in Canada. It is more often found in young adults, women, and people who have never smoked.
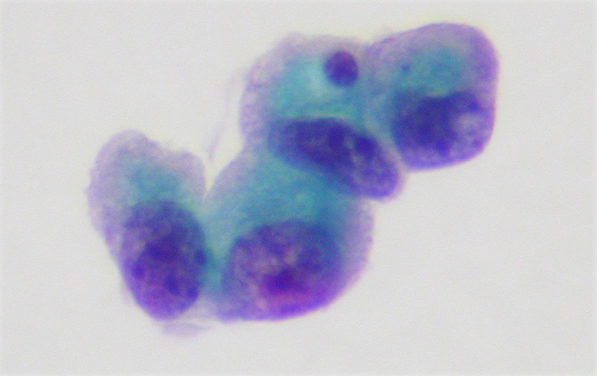
Lung adenocarcinoma usually begins in the outer regions of the lungs. Since these tumours are usually located away from the main airways, symptoms such as coughing and chest pain are less common.
Early symptoms are often subtle. They include shortness of breath during activity, and a general sense of feeling unwell.
Squamous Cell Carcinoma of the Lungs
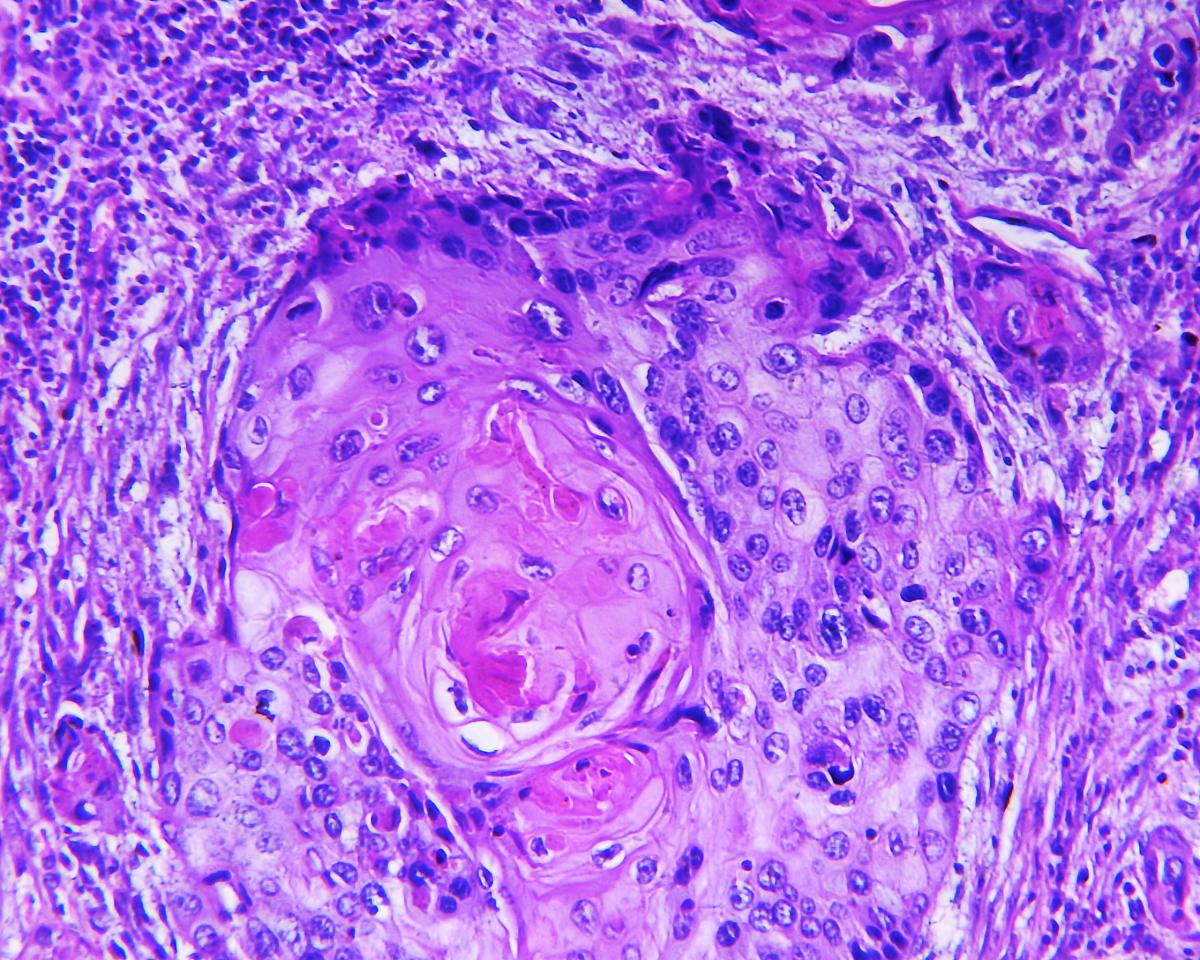
Squamous cell carcinoma of the lung used to be more common, but now accounts for about 30% of non-small cell lung cancers in the Canada.
It usually starts in the main bronchial tubes, in the centre of the lungs.
This cancer is often discovered after people develop a nagging cough, cough up blood, or develop repeated respiratory infections.
Large Cell Carcinoma of the Lungs
Large cell lung cancers are the least common non-small cell cancer. They account for up to 10% of non-small cell lung cancers in the Canada.
Large Cell Carcinoma is an aggressive, and in many cases it behaves like small cell carcinoma.
Over the past decade, there has been a lot of research examining specific genetic mutations of lung cancer cells. These mutations make the cell produce a specific protein that can be targeted with new medications.
These medications can target and destroy the cancer cells with little effect on your normal cells.
There are 2 genetic mutations that you should ask your surgeon about: EGFR, and ALK.
EGFR (Epidermal Growth Factor Receptor)
This protein is expressed on about 50% of patients with adenocarcinoma. This mutation is more common in Asians and in Non-Smokers.
Whether a patient is positive or negative for an EGFR mutation will predict how patients will respond to certain drugs targeted to work against the EGFR mutation, such as Erlotinib (Tarceva ®) or Gefitinib (Iressa ®).
Patients who have an EGFR mutation have a 60% response rate to Erlotinib.
ALK (Anaplastic Lymphoma Kinase)
This mutation is present in 3-5 % of people with non-small cell lung cancer.
STAGING
If cancer cells are found, your surgeon will perform some tests that will help stage your lung cancer.
Stage 1
In this stage, cancer is only in the lung and hasn't spread to the lymph nodes. The tumour is generally smaller than 2 inches (5 centimeters) across.
Stage 2
The tumour may be larger than 2 inches, or it may smaller but has involved nearby structures, such as the chest wall, the diaphragm or the lining around the lungs (the pleura). Cancer may also have spread to the nearby lymph nodes.
Stage 3
The tumour may be very large, and may have invaded other organs near the lungs. Or, this stage may describe a smaller tumour that also has spread cancer cells to lymph nodes farther away from the lungs.
Stage 4
Cancer has spread beyond the affected lung to the other lung or to distant areas of the body.
In some instances, the orginal CT scan may suggest a stage, however, more detailed testing is often required to confirm this. Your surgeon will recommend certain tests to accurately stage the cancer. These tests include:
- PET/CT SCAN
- MRI of the Brain
- Mediastinoscopy/Endobronchial Ultrasound
Mr Ross underwent a PET/CT scan at the MyHealth PET Center. He was in and out within 3 hours.
The results were sent directly to Dr. Irshad and the Nurse Navigator.
A PET/CT scan is not performed within the hospital. Near Osler, there are two locations that perform PET/CT scans for our patients:
KMH Diagnostic Centre
2075 Hadwen Road Mississauga, ON L5K 2L3
MyHealth Centre
6870 Goreway Drive, Suite 101, Mississauga, ON L4V 1P1

You will be asked a few questions prior to your scan. Then you will have your blood glucose levels measured. This is to make sure that the dye injected before the test will be distributed throughout your body well.
After the dye is injected, you will relax for about 45 minutes in a quiet room to allow the dye to travel through your body.
After this, you will lie on a bed and undergo a full body scan. This usually takes between 20-30 minutes. The scan will include low intensity X-ray, CT scan, and PET scan.
Reporting Physicians:
Dr. Nimu Ganguli
Nuclear Radiologist, William Osler Health System
Dr. Marc Freeman
Nuclear Radiologist, Trillium Health Partners
You will be contacted either on the same day or the next day after a requisition is received, and will usually be booked within 2-3 days of this.
Your scan centre will notify the referring physicians about your appointment's date and time.
You will be given all instructions about your appointment during booking and during confirmation.
Your scan centre can fit urgent requests in within 24/48 hours, and will provide referring physicians with Verbal/STAT reports.
The booking line is open daily (Monday - Friday), and requisitions can be sent by fax or via secure email.
Your entire appointment will usually take 1.5-2 hours, and you will leave with a CD containing all the images from your scan.
We can also provide the referring physicians direct access to your PET Scan images.
Written reports are sent to referring physicians within 48 hours.
Paul's scan results showed a nodule in the lower lobe of his right lung that was metabolically active.
There was no activity in the rest of his body. The PET scan could not properly image Paul's brain, so he also underwent a brain MRI, which was normal.
Paul's PET scan showed that his lymph nodes were not active, so he did not require a mediastinoscopy or an endobronchial ultrasound.
In addition to the pulmonary function test, Paul was also scheduled for another tests to make sure his heart was strong enough to withstand major thoracic surgery: a cardiac stress test.
A cardiac stress test is conducted to measure how the heart responds to stress, while the patient is closely monitored in a clinical environment.
During the cardiac stress test
The 'stress' will be caused either by exercise, or through drugs. For exercise-induced stress, will likely be asked to exercsie on a treadmill, or pedal on a stationary bike. If you cannot use your legs you may be asked to pedal a bike-like exercise device with your arms. If the stress is induced chemically, you will receive an intravenous injection that causes the heart to behave similarly to exercise.
During the test, your heart is monitored by an ECG (electrocardiogram), which measures the electrical activity of each heartbeat. Measurements are taken when you are resting, and then during the test when you are at maximum exertion or stress. Comparing these will help your physician determine how well your heart responds to stress, and if there are any conditions to be aware of.
Follow-Up Visit with Thoracic Surgeon
Paul met with Dr. Irshad for his follow-up appointment. Dr. Irshad discussed the elementsof The Thoracic Triangle of Care: Paul's diagnosis, the stage, and his operability.
Diagnosis
Paul's diagnosis was a type of non-small cell lung cancer: adenocarcinoma.
Staging
Paul's tests for staging were good news. They showed no signs of spread beyond the main tumour.
Operability
His tests were good news again! They showed he would tolerate the removal of part of his lung (a lung resection) with low risk.
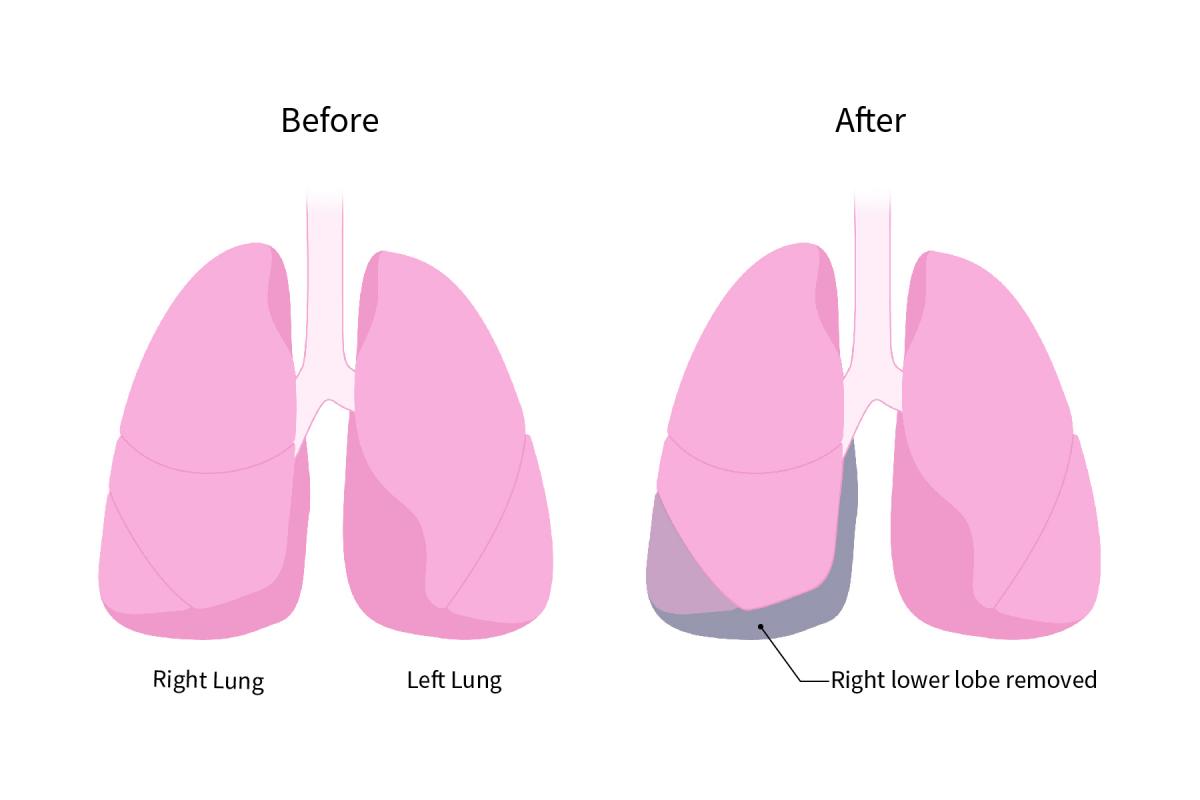
Paul was booked for a minimally-invasive procedure to remove the lower lobe of his rightlung, called a right lower lobectomy or VATS RLL, at the Brampton Civic Hospital.
If Required, Additional Staging Tests
Paul didn't require any additional testing after his initial CT scan, PET/CT scan, CT-Guided needle biopsy, brain MRI, pulmonary function test, and cardiac stress test.
Every patient and case is different. Different or additional tests compared to the tests Paul had might be needed to help your doctors fully and better-assess your own staging.
surgery

Paul arrived 2 hours before his surgery. He changed into a hospital gown and had an IV inserted by the nurse. He also had a small catheter placed into his wrist to monitor his blood pressure.
The Thoracic Surgery team at William Osler Health System:

Our Thoracic Surgery team are pioneers in the field on Minimally Invasive Thoracic Surgery.
In 2006 they were featured on CTV National News introducing Canadians to the benefits to Minimally Invasive Thoracic Surgery for the treatment of Lung Cancer. Below is a clip featured on CTV National News:
No vedio
Dr. Irshad meets with Paul once again before his surgery to discuss his surgical plan
No image
Dr. Irshad discussing the surgical plan with Paul before his surgery
And Paul is ready to go; he is was wheeled into the operating room.

And soon after he is finished being prepped, his surgery is underway.

Paul's surgery went smoothly, with no complications, and Dr. Irshad was able to remove Paul's right lower lobe completely.
Paul's surgery was a success!
After Paul's surgery, the Thoracic Care team was ready to care for him.
Our Physiotherapist ensured that Paul was walking the same day as his surgery, and that he would hopefully be ready for a safe discharge 48-72 hours after his lung operation!

Recovery
Paul was discharged and at home within 2 days of his surgery.
He felt some pain and discomfort during his recovery, but he was able to manage his pain with extra strength Tylenol.
He had an appointment booked in 2 weeks to discuss the pathology results with Dr. Irshad.

Meanwhile in the pathology lab, Dr. Syed Ismael, a top Lung Pathologist in the GTA, analyzed Paul's tumour.

Follow-up for Pathology Results
The pathology results from Dr. Ismael came in, and Paul returned to Dr. Irshad's office to discuss the results.
It's great news! Paul was lucky. He had only Stage 1 lung cancer. The cancer was completely removed during his surgery, and there was no cancer in his lymph nodes.
Paul is cancer free, and doesn't need any further treatment! He will have a check up with Dr. Irshad in 6 months.
Pauls case represents his unique outcome and journey through lung cancer. Everyone's case is unique. You may have a different treatment plan, requiring chemotherapy or radiation before, after, or instead of surgery.
This information is not intended to contradict or replace your physician's advice or personalized treatment plan for you. It is meant to serve as an informational reference to terms, tests, and steps you may encounter on your own journey. You should ultimately consult your own physician on the specific steps in your journey.